Abstract
Editor's Note: The following research article is an accepted manuscript awaiting peer review. Reviews of this article are forthcoming.
Background: Federal rules mandating clinical trial results reporting took effect in 2017 under the Food and Drug Administration Amendments Act (FDAAA) Final Rule, with penalties for non-compliance. While previous studies examined overall reporting rates, this analysis focuses specifically on sponsor-level compliance, providing insights into which institutions are meeting their reporting obligations, and which are falling short.
Methods: This study analyzed FDAAA-mandated trial reporting compliance at the sponsor level for trials completed between 2017-2024. We assessed 12-month compliance and all results reporting rates across different sponsor types (academic medical centers, pharmaceutical companies, and NIH institutes). Sponsors were ranked based on their compliance rates, and trends in improvement or decline were documented.
Results: We identified 257 sponsors listing 10,605 applicable clinical trials during the study period. Overall sponsor compliance with 12-month reporting requirements was 37.2%, with significant variability across institution types. Industry sponsors demonstrated the highest average compliance rates at 73.7%, followed by NIH sponsors at 71.0%, and academic sponsors at 25.5%. The top-performing sponsors across all categories achieved compliance rates exceeding 90%. The IQR reported was between 7.4% and 61.3% for compliance rate. In general, sponsors with fewer clinical trials tended to be much less compliant.
Conclusion: This first comprehensive analysis of individual sponsor-level compliance with FDAAA 801 reporting requirements reveals significant disparities in reporting practices. While some sponsors consistently achieve high compliance rates, many major trial sponsors continue to fall short of legal requirements. These findings highlight the need for targeted interventions to improve compliance among specific sponsors, particularly those with the lowest reporting rates. Achieving higher results reporting should remain a top priority for the FDA and NIH to ensure that scientists can make the most informed decisions when designing and implementing a new clinical trial.
1. Background
Transparency in clinical research is essential for advancing medical knowledge, informing healthcare decisions, and maintaining public trust. The Food and Drug Administration Amendments Act (FDAAA) of 2007 established legal requirements for registering clinical trials and reporting their results on ClinicalTrials.gov, with the Final Rule in 2017 clarifying and expanding these obligations. This regulation took effect with the implementation of the “Final Rule” on January 18, 2017. Under this rule, starting April 18, 2017, responsible parties are required to report trial information.1,2,3,4 Non-compliance penalties may include fines imposed by the FDA, loss of federal grant funding from the NIH, and public disclosure of compliance rates.
Previously, Anderson et al.5 analyzed the ClinicalTrials.gov database prior to 2015 and the 2017 “Final Rule.” These researchers found that only 13.4% of applicable trials (as they defined) were compliant with reporting results within the required 12-month period after clinical trial completion. Riley et al.6 analyzed a database of pulmonary trials during a similar period using the same applicable trials criteria and found a 15% compliance rate. DeVito et al.7 published the first evaluation of compliance rates after the Final Rule was implemented. Their post-2017 study reported a 40.9% compliance rate for results reporting within the one-year deadline.
Previous research by Mughal et al.8 demonstrated modest improvements in overall reporting rates following the implementation of the 2017 Final Rule, with 12-month reporting rates increasing from 8.3% to 23.2%. However, these aggregated statistics mask significant variations in compliance at the sponsor level. Understanding which specific institutions consistently meet or fail to meet their reporting obligations is crucial for targeted enforcement and improvement efforts.
This study represents the first comprehensive analysis of organization-level compliance with ClinicalTrials.gov reporting requirements. By identifying both exemplary performers and consistent underperformers, we aim to promote accountability, recognize best practices, and highlight opportunities for intervention.
2. Methods
2.1 Data Sources
Clinical trial records were obtained from the ClinicalTrials.gov database, focusing on trials subject to FDAAA 801 requirements of HLACTs as defined by Anderson et al.5 then refined by Mughal et al.8 The dataset was accessed with a cut-off date of April 30, 2024.
NIH funding information was obtained from the NIH RePORTER database via ExPORTER9 to identify NIH grantees and analyze compliance patterns among federally funded institutions. This dataset was downloaded on April 15, 2025, and included project funding data from fiscal years 2020 through 2024.
2.2 Inclusion Criteria
Trials were included if they met all of the following criteria:
1. Study record available by the cut-off date of April 30, 2024.
2. Classified as Highly Likely Applicable Clinical Trials (HLACTs) according to established criteria.8 These criteria include applicable clinical trials but do not exclude all non-device, non-drug, or non-biologic intervention trials to closely follow the criteria in [2].
3. Study start date on or after January 18, 2017 (FDAAA 801 Final Rule effective date).
4. Primary completion date between January 18, 2017, and April 1, 2023 (allowing one year for results submission).
Primary completion dates were imputed using the following hierarchy:
1. Primary Completion Date as defined by ClinicalTrials.gov protocol definitions;
2. Study Completion Date (if primary completion date unavailable); or
3. Record Verification Date (if neither primary nor study completion dates are available).
2.3 Sponsor Categorization
Trials were grouped by lead sponsor as reported in ClinicalTrials.gov. Sponsors were classified into mutually exclusive categories based on their lead sponsor class and lead sponsor name in ClinicalTrials.gov:
NIH Sponsors Sponsors with a class of “NIH” in ClinicalTrials.gov were categorized as NIH sponsors. These represent trials directly sponsored by the National Institutes of Health institutes and centers.
Industry Sponsors Sponsors with a class of “INDUSTRY” in ClinicalTrials.gov were categorized as industry sponsors. These include pharmaceutical companies, biotechnology companies, and medical device manufacturers.
Academic Sponsors Academic sponsors were identified using keyword matching algorithms applied to lead sponsor names. Search terms included “University,” “College,” “School of,” “Research Center,” and “Cancer Center” in multiple languages. Additionally, sponsors were required to have a class of “OTHER” to be considered academic.
This categorization is used for computing summary statistics: any lead sponsors that do not fall into these categories are not included in these statistics, as these remaining sponsors do not fit into a single clearly defined group.
2.4 Sponsor Selection for Ranking
To ensure statistical reliability and focus on organizations with substantial research activity, sponsors were required to have a minimum of 9 applicable clinical trials to be included in the primary rankings. This threshold was chosen to provide a sufficient sample size for meaningful compliance rate estimates while maintaining a representative sample of sponsors. Rankings include all sponsors, not just the sponsors that are categorized in Section 2.3.
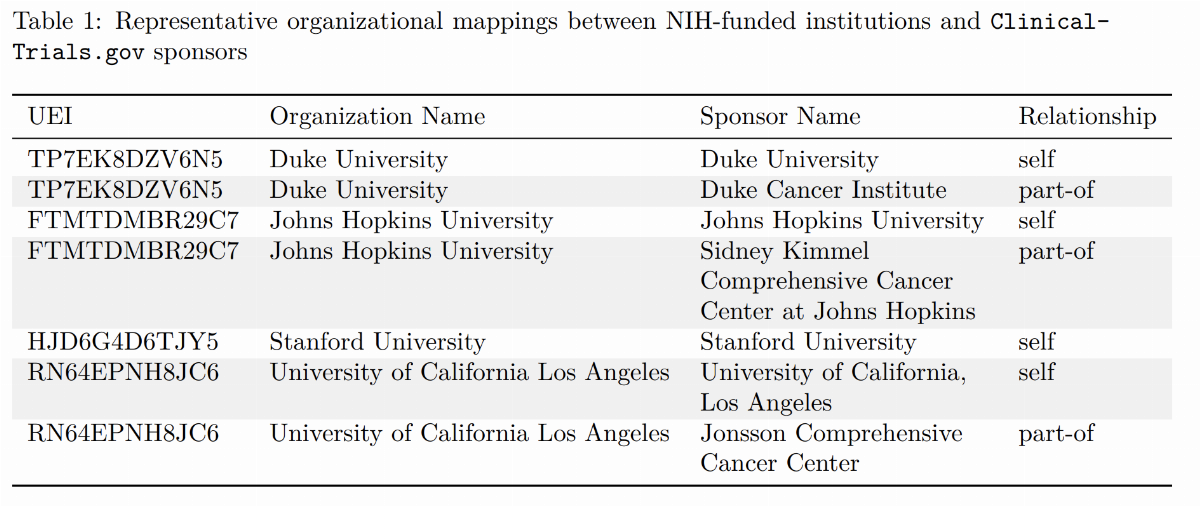
Top NIH-Funded Organizations For the NIH funding analysis, we additionally selected organizations based on their total NIH funding. This approach was implemented by:
1. Extracting the top NIH-funded organizations from RePORTER based on total cost (FY 2020– 2024);
2. Identifying associated NCT IDs from the NIH RePORTER clinical studies table via the NIH RePORTER Core Project Number;
3. Mapping ClinicalTrials.gov lead sponsors and collaborators to NIH RePORTER parent organizations; and
4. Manual curation and verification of organizational relationships.
Table 1 provides representative examples of organizational mappings used in the analysis.
2.5 Statistical Analysis
The following outcomes were calculated for each sponsor:
-Compliance Rate: Proportion of trials with results submitted within 12 months of primary completion date plus any applicable extensions (FDAAA 801 requirement)
-Wilson lower confidence bound (LCB) score: Conservative adjusted estimate of compliance rate used for ranking sponsors
-All Results Reporting Rate: Proportion of trials with results submitted at any time (regardless of timeliness)
Compliance Rate Calculation
For each sponsor, we calculated:

Wilson LCB
To account for varying sample sizes across sponsors, we employed the Wilson lower confidence bound (LCB) score.10 This method provides a conservative estimate of the true compliance rate, such that sponsors with fewer trials (ceteris paribus) have a lower score due to greater statistical uncertainty associated with smaller sample sizes.
The Wilson score was calculated using the prop.test() function in R (version 4.4.1), implementing Wilson’s score interval without continuity correction. The 95% confidence interval lower bound was used for ranking sponsors.
3. Results
3.1 Sponsor-Level Compliance Overall and By Category
We identified 257 organizations sponsoring 10,605 applicable clinical trials completed between 2017 and 2023. The median number of trials per organization was 21.0, with a range of 12.0 to 50.0. Table 2 presents this summary information using the method described in Section 2.3.
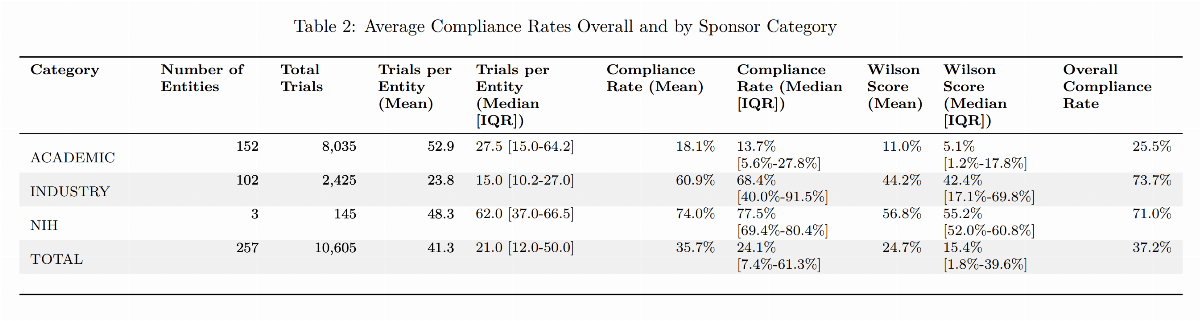
Pharmaceutical and biotechnology companies demonstrated the highest average compliance rates, with an overall compliance rate of 73.7%. Industry sponsors showed the widest variation in compliance rate, with some industry sponsors achieving near-perfect compliance, and the lower quartile of the industry sponsor compliance rate is higher than the upper quartile of the academic sponsor compliance rate.
3.2 Top and Bottom Performers
Table 3 presents the list of the top 10 sponsors by number of trials reported in the analyzed window as described in Section 2.4. Of note, the source of this ranking is all possible sponsors, including those not categorized in Table 2. Mayo Clinic, NYU Langone Health, and Massachusetts General Hospital are not categorized as ACADEMIC sponsors by the method described in Section 2.3; however, the remaining sponsors in this table are all categorized as ACADEMIC.
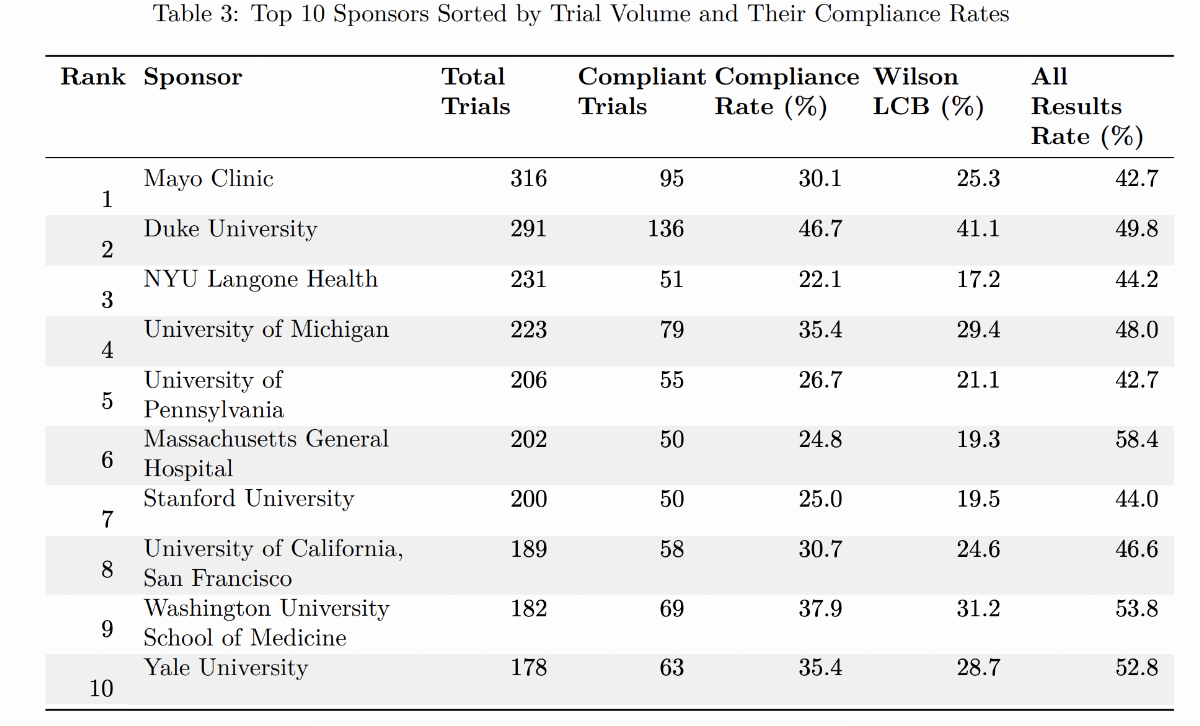
Table 4 lists the top 10 compliant sponsors ranked by Wilson score. Notably, all 10 top compliant sponsors are from industry, with no academic or NIH listed sponsors. This is generally consistent with previous findings that industry sponsors have a higher compliance rate than academic or NIH sponsors. Due to the high compliance rate, there is very little difference between the compliance rate and the all results reporting rate.
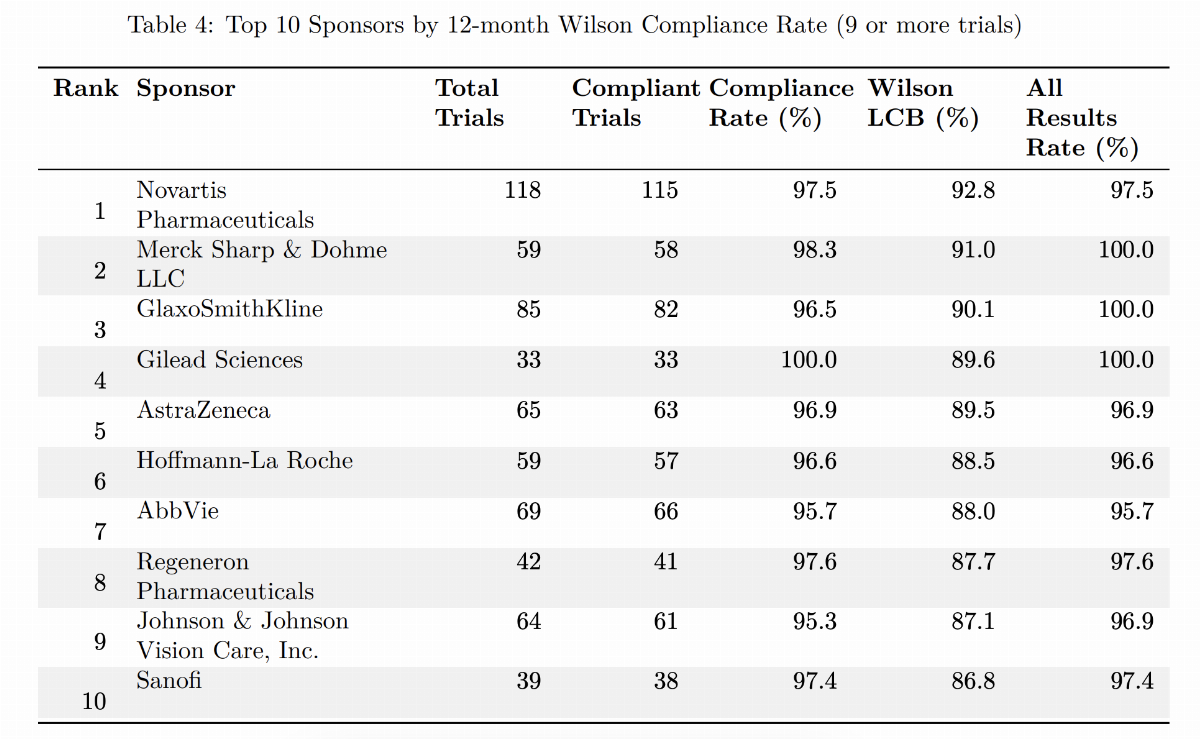
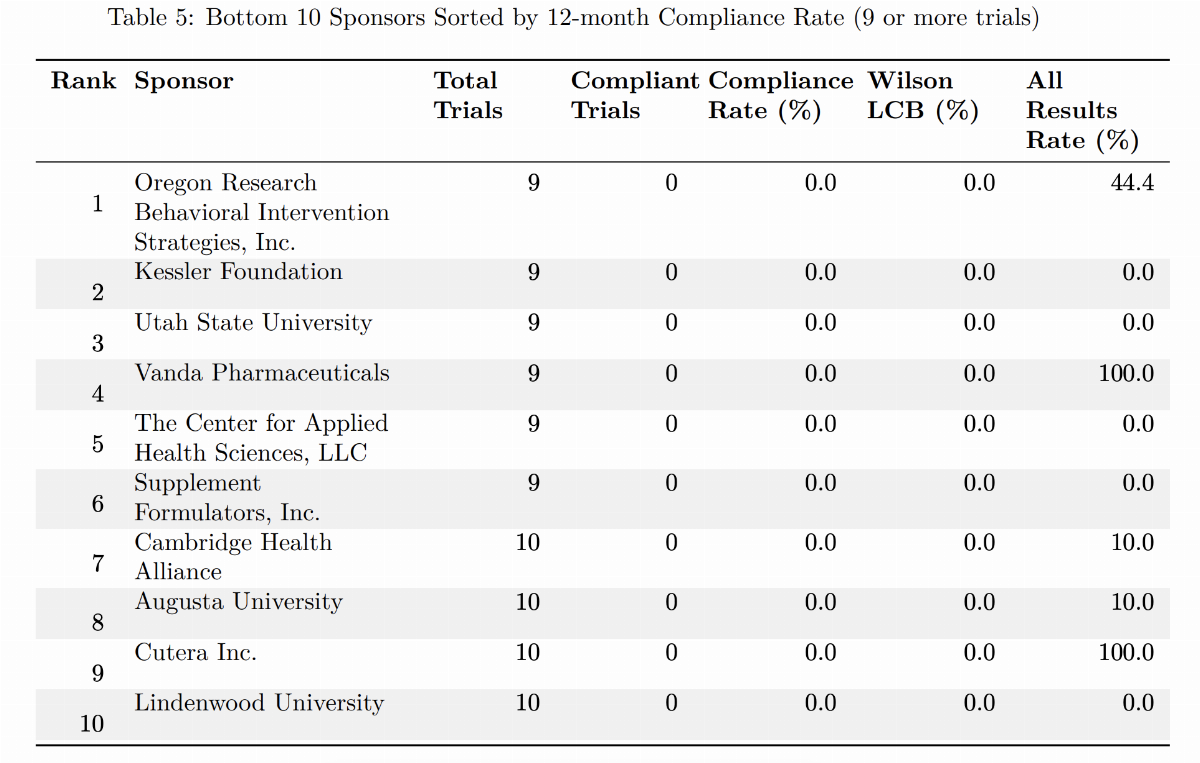
Table 5 reports the bottom 10 sponsors (9 or more trials). Most notably, all of these sponsors have a relatively low number of reported trials, with no sponsor having more than 10 listed trials. While some sponsors eventually reported all results, many sponsors never reported data at any time.
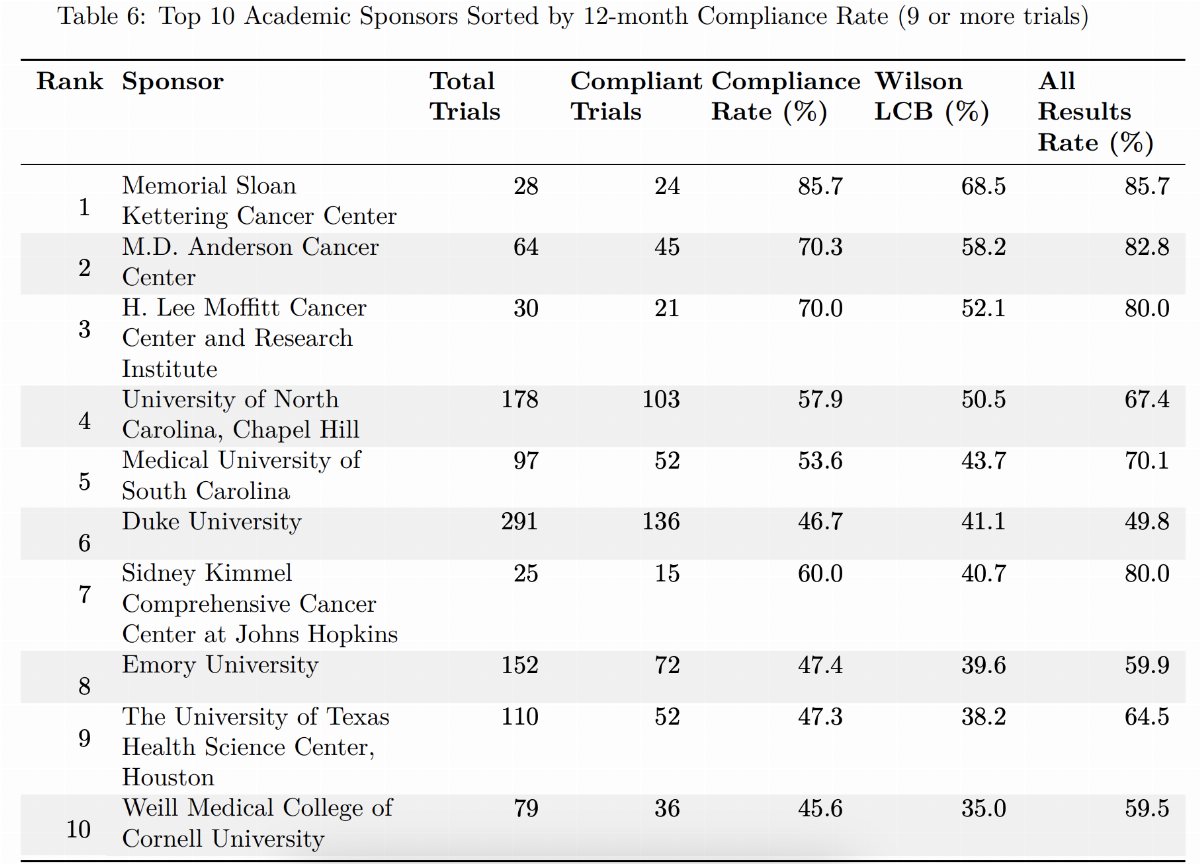
When academic sponsors were sorted for the top 10 most compliant sponsors (Table 6), sponsors’ Wilson scores ranged from 35.0% to 68.5% while the All Results Reporting Rate ranged from 49.8% to 85.7%. These top compliant sponsors tended to have a higher number of listed trials, with only 3 sponsors having fewer than 50 trials listed (Memorial Sloan Kettering Cancer Center; H. Lee Moffitt Cancer Center and Research Institute; and Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins).
4. Discussion
This study provides the first comprehensive analysis of organization-level compliance with FDAAA 801 reporting requirements. Our findings reveal significant disparities in reporting practices across organizations, with some consistently achieving high compliance rates while others repeatedly fail to meet their legal obligations.
4.1 Factors Influencing Organizational Compliance
Several factors appear to influence sponsor compliance rates. Large pharmaceutical companies with established regulatory affairs departments typically demonstrated higher compliance rates than academic or non-profit institutions. This suggests that dedicated resources and expertise for regulatory compliance play a crucial role in meeting reporting requirements.
Sponsors that implemented specific policies and procedures to track trial completion and reporting deadlines achieved significantly higher compliance rates. Examples include automated reminder systems, designated compliance officers, and internal penalties for late reporting.11,12
4.2 Barriers to Compliance
Despite clear federal mandates, many sponsors struggle to consistently report clinical trial results in accordance with regulatory requirements. Interviews with representatives from low-performing institutions reveal several persistent challenges.
Many investigators lack a clear understanding of their legal obligations regarding results reporting. This includes confusion about which trials are subject to mandatory disclosure, the types of data that must be reported, and the deadlines established by laws such as the FDA Amendments Act.11 Without targeted education or ongoing institutional guidance, investigators may undervalue the importance of compliance or misinterpret their responsibilities.
Sponsors may lack adequate systems for tracking trial completion and reporting deadlines. Effective compliance requires robust systems to monitor key trial milestones. However, many sponsors lack centralized infrastructure to track completion dates and alert stakeholders to upcoming reporting obligations. In settings where multiple studies are conducted across different departments, the absence of automated tools or standardized processes significantly increases the risk of missed deadlines.
Low compliance rates may be the result of insufficient staff dedicated to results reporting. Preparing and submitting clinical trial results is a complex, time-consuming task that demands specialized knowledge. Yet, many institutions rely on already overburdened investigators or coordinators to manage this responsibility without dedicated support. The lack of trained personnel often results in delayed or incomplete submissions and diminishes overall reporting quality.
Some sponsors may have overly complex administrative structures that lack accountability. Ambiguous reporting structures within institutions can lead to a lack of accountability. When compliance responsibilities are fragmented or not clearly assigned, critical tasks—such as tracking deadlines or submitting data—can be neglected.11 This diffusion of responsibility is especially problematic in large academic centers or healthcare systems with decentralized governance.
Finally, there likely is a bias toward and concerns about reporting negative results. Cultural and commercial disincentives also hinder compliance. Some investigators may be reluctant to disclose negative or null findings, fearing damage to reputation, reduced publication prospects, or adverse impacts on funding opportunities.11 Sponsors may also resist reporting results they consider commercially sensitive, citing concerns about intellectual property or competitive positioning.
4.3 Implications For Policy and Practice
The wide disparity in compliance rates across sponsors, despite differences in funding source (academia, industry, or NIH), indicates that tailored, sponsor-specific interventions are likely to be more effective than sweeping policy reforms. In fact, for sponsors more reliant upon government funding (Academia and NIH), a very broad and potentially effective but underutilized tool is penalties granted to the FDA and NIH via the FDAAA Act. Our previous report on the effect of this legislation was positive but incremental, with a remaining gap in data reporting. Therefore, going forward, we recommend a combination of efforts to enhance compliance by prioritizing enhanced education of institutions with low reporting performance while focusing on legally authorized penalties for sponsors with a greater number of trials and greater NIH funding. Sponsors with low reporting performance often have fewer clinical trials. A reasonable conclusion is that these sponsors lack the knowledge and resources required for compliant reporting. Several targeted strategies could help close this gap, including increased transparency and accountability, standardized reporting protocols, improving education of deficient entities, providing improved technical support, utilizing existing statutory enforcement authority, and providing rewards for improved performance.
Increasing transparency and accountability can be achieved by publicly sharing sponsor-level compliance data, which can motivate improvement by highlighting disparities and placing reputational pressure on underperforming institutions.
Developing clear, user-friendly, and standardized reporting templates and processes, especially for academic and non-profit sponsors, can streamline compliance and reduce administrative burden.
ClinicalTrials.gov should offer specialized assistance to institutions lacking regulatory expertise, which can help overcome knowledge gaps and build internal capacity for timely and accurate reporting.
As a consequence of the 2017 FDAAA, regulatory authorities at the FDA and NIH possess potent punitive tools to enforce compliance. These tools should be used. The FDA has rarely used its authority to penalize non-compliant entities,13,14 while there are no reports of NIH using its statutory authority to withhold grant money from non-compliant entities. Consistently applying penalties, especially for sponsors with repeated violations, reinforces the importance of compliance and deters negligence.
Finally, imposing punitive incentives is best matched with positive reward actions. Introducing incentives for sponsors with strong compliance records, such as eligibility for expedited reviews or preferential consideration in funding decisions, can reinforce positive behavior and establish a culture of accountability.
4.4 Limitations
This study has some limitations. First, our identification of applicable trials relied on the algorithm developed by Anderson et al., which may not capture all trials subject to FDAAA requirements. This definition of applicable clinical trials does not exactly fit the definition of trials covered in the FDAAA legislation, and therefore, sponsor non-compliance should not be interpreted in a legal context. However, we conducted an analysis using a refined definition aligning with the legal definition of applicable trial, and the results did not differ appreciably. We believe that the broader definition of applicable clinical trials is more relevant from an ethical and scientific perspective. Second, the publicly available ClinicalTrials.gov database was used for all analysis, and not the private PRS database for each sponsor, which may have updated data that we are unaware of. Finally, changes in sponsor names, mergers, and acquisitions may have affected the attribution of trials to specific sponsors over time.
5. Conclusion
Our findings demonstrate that while some sponsors consistently achieve high compliance with FDAAA reporting requirements, many major trial sponsors continue to fall short of their legal obligations. Publishing sponsor-specific compliance rates provides transparency and accountability that may drive improvements in reporting practices.
Future research should examine the specific policies and practices that distinguish high-performing sponsors from those with poor compliance, as well as the effectiveness of targeted interventions to improve reporting rates among consistent underperformers. Achieving higher results reporting should remain a top priority for the FDA and NIH to ensure that scientists can make the most informed decisions when designing and implementing a new clinical trial.
6. Supplement
6.1 Academic Sponsors –– Full Ranking by Wilson Score And Including the Compliance Rate and All Results Reporting Rate
References
FDAAA 801 and the Final Rule. ClinicalTrials.gov. 2024 Apr 30. Available from: https: //clinicaltrials.gov/policy/fdaaa-801-final-rule [Accessed on: 2024 Sep 25]
Zarin DA, Tse T, Williams RJ, and Carr S. Trial Reporting in ClinicalTrials.gov — The Final Rule. New England Journal of Medicine. 2016 Nov 17; 375:1998–2004. doi: 10.1056/ NEJMsr1611785. Available from: https://www.nejm.org/doi/full/10.1056/NEJMsr1611785
National Institutes of Health, Department of Health and Human Services. Clinical Trials Registration and Results Submission. 2014 Nov 21. Available from: https://www.federalregister. gov/documents/2014/11/21/2014-26197/clinical-trials-registration-and-resultssubmission [Accessed on: 2024 Nov 20]
Clinical Trials Registration and Results Information Submission. 42 CFR Part 11. 2017 Jan 18. Available from: https://www.ecfr.gov/on/2017-01-18/title-42/part-11 [Accessed on: 2024 Nov 20]
Anderson ML, Chiswell K, Peterson ED, Tasneem A, Topping J, and Califf RM. Compliance with Results Reporting at ClinicalTrials.gov. New England Journal of Medicine. 2015 Mar 12; 372:1031–9. doi: 10.1056/NEJMsa1409364. Available from: https://www.nejm.org/doi/ full/10.1056/NEJMsa1409364
Riley IL, Boulware LE, Sun JL, Chiswell K, Que LG, Kraft M, Todd JL, Palmer SM, and Anderson ML. Factors associated with reporting results for pulmonary clinical trials in ClinicalTrials.gov. Clinical Trials (London, England). 2018 Feb; 15:87–94. doi: 10.1177/1740774517740352
DeVito NJ, Bacon S, and Goldacre B. Compliance with legal requirement to report clinical trial results on ClinicalTrials.gov: a cohort study. Lancet (London, England). 2020 Feb 1; 395:361–9. doi: 10.1016/S0140-6736(19)33220-9
Mughal Z, Fu R, Luechtefeld T, Chiswell K, Kleinstreuer N, Shaw G, and Tidmarsh GF. Compliance with Results Reporting at ClinicalTrials.gov Before and After the 2017 FDAAA Final Rule: A Comparative Analysis. RealClearJournals 2025. doi: 10.70542/rcj-japh-artvr3aga. Available from: https://doi.org/10.70542/rcj-japh-art-vr3aga
National Institutes of Health. ExPORTER. 2025. Available from: https://reporter.nih. gov/exporter [Accessed on: 2025 Apr 15]
Wilson EB. Probable Inference, the Law of Succession, and Statistical Inference. Journal of the American Statistical Association 1927; 22:209–12. doi: 10.1080/01621459.1927.10502953
Improving Timely, Accurate, and Complete Registration and Reporting of Summary Results Information on ClinicalTrials.gov. Clinical Trials Transformation Initiative, 2024 Jan 10. Available from: https://ctti-clinicaltrials.org/topics/quality/reporting-challenges/ ctti- and- fda- share- strategies- for- improving- timely- accurate- and- completeregistration- and- reporting- of- summary- results- information- for- applicableclinical-trials-on-clinicaltrials-gov/ [Accessed on: 2024 Oct 2]
Office of Inspector General. The National Institutes of Health Did Not Ensure That All Clinical Trial Results Were Reported in Accordance With Federal Requirements. A-06-21-07000. U.S. Department of Health and Human Services, Office of Inspector General, 2022 Aug 12. Available from: https://oig.hhs.gov/reports/all/2022/the-national-institutes-of-healthdid-not-ensure-that-all-clinical-trial-results-were-reported-in-accordancewith-federal-requirements/ [Accessed on: 2024 Oct 2]
Office of the Commissioner. ClinicalTrials.gov - Notices of Noncompliance and Civil Money Penalty Actions. FDA. 2023 Dec 20. Available from: https://www.fda.gov/scienceresearch/fdas- role- clinicaltrialsgov- information/clinicaltrialsgov- noticesnoncompliance-and-civil-money-penalty-actions [Accessed on: 2024 Oct 11]
Tanne JH. US Drug Regulator Issues Its First Ever Non-Compliance Notice for Not Posting Trial Results. BMJ. 2021 May 28; 373:n1384. doi: 10.1136/bmj.n1384. pmid: 34049852. Available from: https://www.bmj.com/content/373/bmj.n1384 [Accessed on: 2024 Oct 11]
