Abstract
Overwhelming evidence shows that exposure of susceptible babies and children to acetaminophen (paracetamol) triggers many if not most cases of autism spectrum disorder, and that oxidative stress causes susceptibility. However, these conclusions have not yet been widely acknowledged or integrated into clinical practice or regulatory guidelines, leaving the continued high prevalence of autism spectrum disorder unchecked. To understand why the conclusions have not been widely accepted, this study conducts systematic analyses of all PubMed-indexed papers with “acetaminophen” and “autism” in any search field. In these papers, statements that failed to promote changes in clinical practice or regulatory guidelines were pervasive. Also pervasive were mishandlings of available evidence, including treating interacting variables as if they are confounding factors (66% of studies affected) and considering too narrow a range of evidence (77% of studies affected). Also present were erroneous criticisms of potentially groundbreaking research, undermining the potential impact of that research. It is hoped that identification of these fundamental problems will lead to widespread acceptance of the evidence that acetaminophen triggers autism spectrum disorder in susceptible babies and children and to subsequent regulatory and clinical changes that will effectively and quickly reduce the induction of autism spectrum disorder.
Introduction
Based on overwhelming evidence, we have previously concluded that exposure of susceptible babies and children to acetaminophen (paracetamol) causes many if not most cases of autism spectrum disorder (autism).1,2,3,4 Further, we concluded that susceptibility is imparted by inflammation and oxidative stress, which can be caused by a wide range of genetic, epigenetic and environmental factors.5 In addition, we concluded that acetaminophen is likely involved in the etiology of the vast majority of cases of autism,2 a compelling view from a scientific perspective as it satisfies Occam’s Razor,5 and a compelling view from a public health perspective as it holds the key to a profound and readily obtainable reduction in the prevalence of autism. Further, we have previously determined that the time window for risk of acetaminophen-mediated induction of autism likely starts sometime during pregnancy4 and, possibly with rare exceptions, ends by the age of 5 or 6 years, with the most sensitive period being the peripartum period after the umbilical cord is clamped.4
We have recently reviewed evidence pointing toward the induction of autism following exposure of susceptible individuals to acetaminophen.1,2,3,4 To summarize, while no single line of evidence is, by itself, convincing, the body of evidence considered as a whole is sufficiently compelling. That body of evidence includes over two dozen lines of evidence from clinical observations, laboratory animal studies, pharmacologic considerations, and multiple, independent associations through space, time and human behavior.2,3 The body of evidence, when considered as a whole, indicates that autism is a hallmark of acetaminophen exposure during neurodevelopment in the presence of oxidative stress. That same body of evidence effectively rules out trivial explanations for increases in autism such as changing awareness and diagnostic criteria, accepting that a profound increase in the incidence of autism over the past century has led to improved diagnosis and awareness, as might be expected.
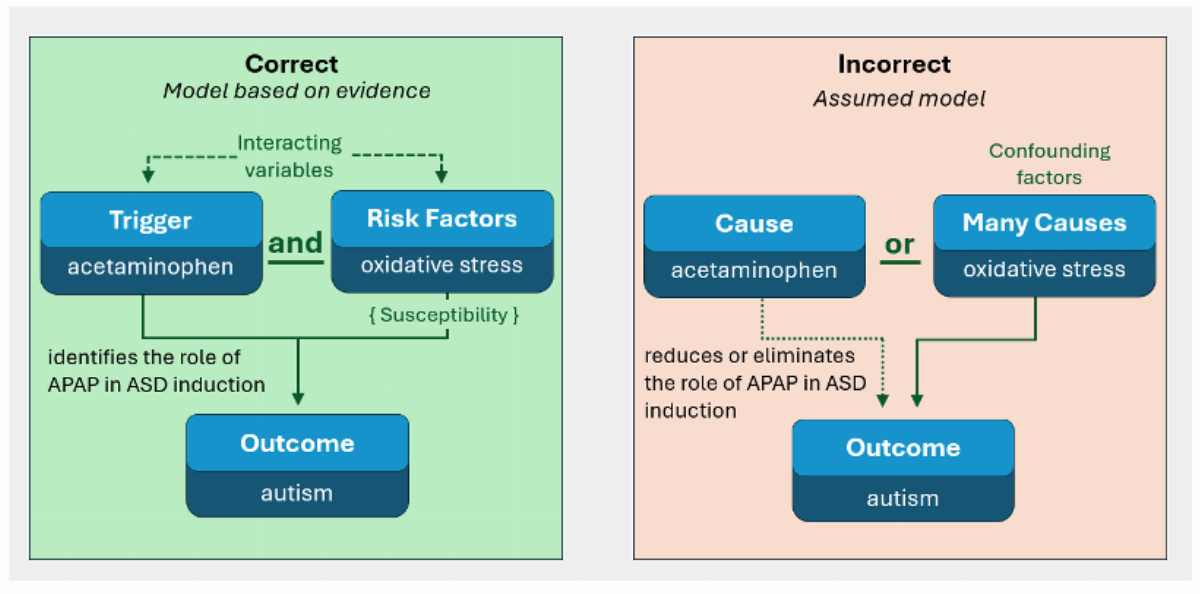
Despite overwhelming evidence, current medical literature in the field adheres to the myth that autism has a complex cause, with multiple factors contributing to the disorder, and with no single factor being critical.2 This myth, like many myths, contains some elements of reality. Evidence does indeed demonstrate that oxidative stress, a cofactor in the acetaminophen-mediated induction of autism, has a complex underpinning, with multiple genetic and environmental factors contributing.5 However, the myth misses the role of acetaminophen as a single, critical factor to the induction of autism, and thus stands as an impediment to progress in reducing the prevalence of autism. The myth itself is founded upon a widely known error in science: the fact that many risk factors are associated with autism does not mean that those many risk factors cause autism. Association does not equal causation.
It might be argued that strong evidence that acetaminophen triggers autism in susceptible babies and children has only recently emerged, accounting for the current lack of awareness of the ongoing and widespread induction of autism. However, evidence does not support this view. The first study specifically probing the association between acetaminophen and autism was published in 20086 by Schultz and colleagues, finding that use of acetaminophen in early childhood was associated with regressive autism. This observation provided grounds for a newly minted hypothesis that, in hindsight, was supported by numerous lines of evidence already present in the scientific literature prior to 2008. Much of that evidence was pointed out by Good in 2009.7 For example, the prevalence of autism had been rising sharply since 1982 after aspirin was replaced with acetaminophen due to concerns about Reye syndrome, a fact known by 1987.8 Further, it was found in the 1990s that children with autism could not efficiently metabolize acetaminophen,9 rendering them susceptible to enhanced production of the toxic metabolite of acetaminophen, which had itself been well described by the 1970s.10 In addition, veterinary science literature in the 1980’s supported the view that administration of acetaminophen to domestic cats was ill advised due to metabolic deficiencies that lead to enhanced toxicity.11,12,13 The same metabolic deficiencies had been known since the 1970s to exist in human neonates.14,15 As another example, a literature review prior to 1990, had it been performed, would have revealed that the presumed safety of acetaminophen for pediatric use was based solely on studies monitoring liver function,16 but studies in the 1980s had demonstrated that even lethal doses of acetaminophen do not cause significant liver damage in neonatal laboratory mice17 or in domestic cats,13 which have limitations affecting acetaminophen metabolism similar to those found in human neonates. Further, the fact that a drug which profoundly affects biosynthetic pathways in the human brain was not tested for its impact on neurodevelopment even in laboratory animals seems reckless and would have been evident even in the 1970s as acetaminophen was being considered for widespread use in neonates.
As another example of evidence connecting acetaminophen and autism prior to 2008, parents for decades have attributed their child’s autism to vaccination,18,19,20,21 and that attribution was noted years prior to 2008.22,23 Indeed, what motivated the 2008 study by Schultz and colleagues6 was Schultz’s observation that his son’s regression into autism coincided with administration of the MMR vaccine.24 Schultz et al6 found that acetaminophen use during childhood, including administration with the MMR vaccine, was strongly associated with regressive autism, providing an explanation for parents’ observations, including his own. Importantly, given frequent use of acetaminophen with vaccination, the parents’ observations that vaccination and regression into autism are associated can then be considered as another line of evidence linking acetaminophen with autism. Again, while that evidence alone is not overly convincing, it should be considered as part of the larger body of evidence.
As we have described previously in some detail,5 observations of parents have historically been extremely useful, and main-stream medicine has historically suffered when those observations were disregarded. That disregard led to two decades of acceptance of the tragic “refrigerator mother” hypothesis, followed by four decades of belief that regressive autism was not possible, an idea finally disproven in 2005.25 Thus, while the study by Schultz et al in 2008 was not, by itself, overwhelmingly convincing that acetaminophen and autism were connected in a causal manner, it did offer a plausible explanation for the observations of many parents who attributed their child’s autism to vaccination.
The several lines of evidence available prior to 2008, including the observations of parents, temporal associations, and various metabolic considerations, taken together did support a causal link between acetaminophen and autism. That body of evidence in 2008, though perhaps not overwhelming, was certainly concerning and should have driven immediate changes in clinical practice and regulatory guidelines followed by intensive research efforts. Immediate research efforts should have included work evaluating the impact of acetaminophen on neurodevelopment in neonatal laboratory animals, which had, unfortunately not been conducted prior to approval of the drug for use in babies and children. Indeed, when such work was eventually conducted, in 2013 at Uppsala University by Viberg and colleagues,26 it showed conclusively that acetaminophen is a developmental neurotoxin.
The goal of this work is to probe potential reasons why evidence pointing toward the acetaminophen -mediated induction of autism, much of it now more than a decade old, has been considered insufficient to stimulate change in clinical practice and regulatory guidelines. In order to accomplish this goal, views expressed in the published literature regarding acetaminophen -mediated induction of autism were assessed, and the rationale underpinning those views was evaluated.
Methods
Overall approach
To gain insight into why the medical literature has failed to consistently support changes in clinical practice and regulatory guidelines based on convincing evidence that many if not most cases of autism are triggered by acetaminophen in susceptible babies and children, the PubMed-indexed literature addressing the role of acetaminophen in autism was evaluated. Two sets of manuscripts were evaluated. First, all papers in PubMed that included the words “autism” and either “acetaminophen” or “paracetamol” in any search field were evaluated. Second, seminal studies contributing to current understanding of the connection between acetaminophen and autism were selected as described below, and PubMed-indexed studies listed as citing those studies were evaluated. This two-pronged approach facilitated assessment of the scientific literature in general, and assessment of the handling of specific lines of evidence related to the connection between acetaminophen and autism.
Papers were analyzed to identify previously reported mishandling of evidence that may have impeded the authors of those papers from observing the role of acetaminophen in the induction of autism. First, the presence or absence of a statistical error made in dealing with “potentially confounding factors” was documented in each paper. This type of mishandling has been described in detail previously2 and is summarized in the relevant section in Results, below. A second type of mishandling which can impede authors from observing evidence pointing toward the induction of autism by acetaminophen is a failure to consider the entire time window of susceptibility to acetaminophen -mediated neurodevelopmental injury. This type of mishandling has been previously documented,4 and the presence or absence of this problem was documented in all papers evaluated. While it is recognized that data collection and evaluation in many papers is necessarily limited to a narrow time period of sensitivity (e.g., the peripartum period or during pregnancy), it is also expected that any medically relevant Discussion of the role of acetaminophen in neurodevelopment will describe study data in context with other evidence in the field.
All studies published by one or more of the coauthors of this manuscript were excluded to avoid biasing the results. The two errors described above were identified and categorized by two coauthors independently, with a third coauthor adjudicating any differences between their evaluations (see the Methods in the Supplemental File, including Supplemental Figure 1 and Supplemental Table 1 for additional details on the article selection and assessment process).
Systemic evaluation of all articles containing the terms autism and acetaminophen in any PubMed search field
All papers in PubMed that included the words “autism” and either “acetaminophen” or “paracetamol” in any search field were assessed as described above. In addition, all statements made about acetaminophen’s contribution to neurodevelopmental disorders were systematically binned into specific categories that ranged from the conclusion that acetaminophen is a neurodevelopmental toxin to acetaminophen is not a neurodevelopmental toxin. The majority of papers fell into the middle ground, describing some current evidence, but either suggesting that the evidence is not conclusive (one bin) or is weak (another bin). Statements which included disclaimers such a “maybe”, “might”, “suggests”, “potentially”, or “possibly” were considered to be inconclusive in nature and were classified as accepting that some evidence of risk of acetaminophen for neurodevelopment exists, but that the evidence is not conclusive. Whether authors called for safety reevaluation, change in clinical practice, or more studies was documented. (see the Methods in the Supplemental File for additional details on methods of identifying and categorizing statements made in all manuscripts.)
In light of conclusive evidence regarding the role of acetaminophen in the development of autism, statements were categorized as “helpful” if they promoted an immediate change in clinical practice or work toward regulatory change. Statements were classified as “futile” if they called for caution in use without any specific suggestion for change, called for more studies to address unresolved issues, or made qualified statements that some evidence of risk of acetaminophen for neurodevelopment may exist, without calling for any change in clinical or regulatory practice. “Harmful” statements, on the other hand, were considered those that reduced or assuaged concerns regarding the risk of acetaminophen for neurodevelopment. As described in more detail in the Results section, classification of a statement as futile or harmful did not necessarily reflect technical inaccuracy, but did reflect potential harm from a practical perspective. Such statements presented a distorted view of the neurodevelopmental impact of acetaminophen, either as a result of systematic scientific errors or by focus on a very narrow time frame that did not consider the broader picture of the neurodevelopmental impact of acetaminophen.
Treatment of seminal studies in the field by subsequent work
As a second approach to evaluating problems that have prevented acceptance of the role of acetaminophen in autism, the treatment of seminal work in the field was assessed. For this purpose, a panel of five individuals, including two coauthors, two technicians and one ad hoc member (see acknowledgements), selected three specific studies as providing “the most compelling, stand-alone evidence of the risks of acetaminophen exposure in susceptible individuals for neurodevelopmental problems”. The three studies selected for targeted analysis included two hypothesis driven research efforts looking at the connection between acetaminophen and autism in humans, one looking at autism and acetaminophen use with vaccination, published in 2008,6 and the other evaluating autism and circumcision, a procedure commonly associated with acetaminophen exposure, published in 2015.27 The third article selected for further analysis was the first study showing profound, acetaminophen-mediated neurodevelopmental problems in laboratory animals, published in 2013.26 All papers listed in PubMed as citing any of those three studies were assessed as described in the General Approach section. In addition, conclusions made in those papers regarding the role of acetaminophen in neurodevelopmental disorders were systematically binned into specific categories that ranged from the conclusion that acetaminophen is a neurodevelopmental toxin to acetaminophen is not a neurodevelopmental toxin. Whether authors called for safety reevaluation, change in clinical practice, caution in use, or more studies was documented. Statements which included disclaimers such a “maybe”, “might”, “suggests”, “potentially”, or “possibly” were considered to be inconclusive in nature and were not tallied.
Results
Predominance of statements in the medical literature either of questionable utility or not helpful from a clinical perspective
Out of 84,454 articles in PubMed with the term “autism” in any search field published in any year, 64 articles contained the terms “acetaminophen” or “paracetamol” in any field and discussed the safety of acetaminophen for neurodevelopment. These 64 studies were submitted to further evaluation, identifying statements regarding the role of acetaminophen in the induction of neurodevelopmental disorders. (See Supplemental Table 2 for statement assessments in all manuscripts.)
The 64 studies considering the safety of acetaminophen for neurodevelopment spanned an 18-year time frame, from 2008 to 2025. The summary data in Figure 1 indicate that, during that 18 years, no significant shift in opinions or conclusions regarding the safety of acetaminophen for neurodevelopment has occurred. It could be argued that, in 2008 when the connection between acetaminophen and autism was first proposed,6 evidence was much weaker than it is at the present time. However, that proposal, if it had been taken seriously at that time, would have led to a thorough investigation. That investigation, if it had been conducted at that time, would have revealed a considerable body of compelling evidence already in existence in the medical and scientific literature pointing toward a critical role of acetaminophen in the induction of autism. The body of evidence available prior to 2008 is addressed in some detail in the Introduction. The weight of that evidence available at that time indicates that the risk of acetaminophen for neurodevelopment should have been profoundly concerning, even at that time. Further, given that acetaminophen has no proven long-term benefits, the precautionary principle should be in effect. If evidence of significant and widespread harm exists without any evidence of long-term benefit, the drug should not be used.

In light of conclusive evidence regarding the role of acetaminophen in the development of autism, statements were categorized as “helpful”, “futile, or “harmful” from a practical perspective focused on needed changes in clinical practice or regulatory guidelines (Figure 1). Statements deemed helpful promoted an immediate change in clinical practice or work toward regulatory change that would decrease exposure to acetaminophen during neurodevelopment. Fifteen papers with fifteen such statements were found (Figure 1) in the literature. These statements either concluded that acetaminophen is toxic for neurodevelopment (n = 1), called for a change in medical practice (n = 8), or called for a drug safety re-evaluation (n = 6). Thus, less than one out of every four papers (15/64, 23%) contained a statement or statements that were deemed helpful in promoting changes in clinical practice or regulatory guidelines that are mandated by evidence regarding the critical role of acetaminophen in the development of autism and perhaps other neurodevelopmental disorders. However, two of the papers with helpful statements did not focus on acetaminophen in particular, but rather on multiple environmental exposures (Figure 1), decreasing the potential usefulness of those statements in terms of driving specific changes in clinical practice related to acetaminophen use.
Statements deemed futile for practical intents and purposes were by far the most common. Such statements did not call for a meaningful change in clinical practice or regulatory action, although they often acknowledged that some evidence of risk for acetaminophen use exists. A call for “caution in use” of acetaminophen was made 8 times, although such calls for caution do not support any specific modifications to standards of care or recommendations for regulatory change that could potentially affect over-the-counter use of the drug. Thus, these statements were considered futile since they do not mandate immediate and profound changes in clinical practice and regulatory guidelines that are based on current evidence (for reviews, [1-4]). More than 60% of all articles (40/64, 63%) concluded that more studies need to be conducted to address unresolved issues. A similar number (39/64, 61%) used disclaimers such as “maybe”, “might”, “possibly”, or “potentially” in describing the neurodevelopmental impact of acetaminophen. These papers are listed in Figure 1 as accepting that “some evidence of risk” of acetaminophen for neurodevelopment exists, although that evidence was considered inconclusive, a view inconsistent with the overwhelming nature of current evidence. While it is recognized that such statements might be considered technically accurate since no absolute proof of the induction of autism by acetaminophen has been produced, these statements are considered futile from a practical perspective since they are not expected to encourage immediate changes in clinical practice or regulatory guidelines.
A total of 15 statements from 14 papers were found which were considered harmful from a clinical or regulatory perspective (Figure 1) since the statements might discourage changes in clinical practice or regulations regarding the use of acetaminophen during neurodevelopment. Although unlikely, it was possible that statements considered harmful were not necessarily wrong from a technical perspective. For example, the view that weak evidence supports a causal relationship between acetaminophen use during early pregnancy and autism is probably defensible from a technical perspective, but this statement does not address the bigger picture of the role of acetaminophen in the induction of other neurodevelopmental disorders during pregnancy, or the induction of autism at other times, particularly during the last hours of pregnancy4,28 and up until early childhood.4 Thus, statements that focused on a lack of evidence of harm within a limited context, without consideration of a wider picture, were considered harmful from the practical perspective without regard for technical accuracy.
Harmful statements described conclusions that insufficient evidence of risk from acetaminophen exposure exists (n = 6), that no evidence of risk of acetaminophen exposure exists (n = 7), that risk from acetaminophen exposure is unlikely (n = 1), or that considerable evidence exists showing that acetaminophen is safe for neurodevelopment (n = 1).
Mishandling of evidence 1: The prevalent and fundamental statistical error of assuming interacting variables are confounding factors
One common and unfortunately profound way that data pertaining to the safety of acetaminophen for neurodevelopment is mishandled is the fundamental statistical error of treating interacting variables as confounding factors. Since the error was first introduced in 2013 to the analysis of the neurodevelopmental effects of acetaminophen,29 it has affected 82% (45 out of 55) of PubMed-indexed studies discussing the safety of acetaminophen for neurodevelopment either in their own analysis or in papers considered in the introduction or the discussion of their paper (Supplemental Table 2). All three studies published in 2025 were affected by this error.
Currently available evidence establishes that oxidative stress interacts with acetaminophen in the induction of autism. In other words, acetaminophen triggers autism not on its own, but in conjunction with oxidative stress, with oxidative stress creating the condition of susceptibility (Figure 2). However, all studies in the literature analyzing healthcare databases for the effects of acetaminophen incorrectly treat variables leading to oxidative stress as confounding factors.30 By “adjusting for” factors related to oxidative stress in this way, these studies inadvertently hide the effects of acetaminophen in conjunction with oxidative stress. This problem is particularly severe if acetaminophen is widely used by susceptible and non-susceptible individuals,1 and worsened further if some measures of acetaminophen exposure are not accurate or complete.2
An example of the impact of adjustment for oxidative stress-related factors can be seen in interpretations of laboratory animal studies. For example, Viberg and colleagues reported in 2013 the first observations of adverse neurodevelopmental impacts of acetaminophen in laboratory animals,26 finding a profound, long-term loss of ability to find food in a maze following two doses of 30 mg/kg acetaminophen received four hours apart during the first days of life. This dose of acetaminophen is lower than the 40 mg/kg received by some children receiving acetaminophen via suppositories, and thus the results should have been of considerable concern. However, most studies citing Viberg’s paper (31/39, 79%) were overtly affected by studies incorrectly adjusting for potential confounding factors (Supplemental Table 3).
In a specific example of the influence of invalid adjustment for confounding factors, in 2018 Blecharz-Klin and colleagues31 observed a ten-fold increase (p < 0.005) in wrestling behavior in rats exposed to sub-therapeutic doses (15 mg/kg/day) of
acetaminophen during fetal development. By comparison, humans, regardless of age, can receive approximately 15 mg/kg oral acetaminophen every four to five hours for indefinite periods of time. This 10-fold increases in wrestling should have been alarming, but Blecharz-Klin and colleagues state that “Most studies do not provide strong support for a change in clinical practice regarding the use of paracetamol by pregnant women”, citing studies that adjust for oxidative-stress-related variables in analyzing human health data for risks of acetaminophen exposure.
Given the role of oxidative stress in the induction of acetaminophen-mediated neurodevelopmental injury,5 and given the very broad range of factors that can be associated with oxidative stress,5 it is potentially an error to assume that any factor is “confounding” in the acetaminophen-mediated induction of autism. Examples of oxidative stress related factors include poverty32 and a variety of other issues associated with socioeconomic status,33 many medications, including morphine,34 which can be used during cesarean sections, and antibiotics,35 heavy alcohol use,36 smoking,36,37, an elevated BMI,38 and genetics.39,40 The number of children a woman has borne apparently affects oxidative stress responses during pregnancy,37 and a number of common medical conditions, including depression41,42,43 and infections,44,45 are directly related to oxidative stress.
With the above in mind, it is apparent that any valid analyses of healthcare databases or of data from any cohort for associations between acetaminophen use and autism must avoid assumptions regarding the presence or absence of confounding factors. While this rule limits the conclusions that can be drawn from such analyses, we have argued that other evidence, abundant in nature, is more than sufficient to draw conclusions regarding the causal relationship between acetaminophen use and autism.2
Mishandling of evidence 2: Small fraction of available evidence used to draw conclusions
A second common way that data are mishandled is that only a fraction of available evidence is relied upon to draw conclusions. Only 15 studies (15/64, 23%), for example, considered evidence related to acetaminophen risks during pregnancy, the peripartum period, and the postnatal period (Supplemental Table 2). The distinction between these three time periods is important because each time period involves potentially different reasons for exposure to acetaminophen, different medical specialties, potentially different levels of sensitivity to acetaminophen-mediated injury,4 and different sources of data and evidence. Evidence regarding the neurodevelopmental risks of acetaminophen during pregnancy, the peripartum period and the postnatal period became available in 2013,29 2013,46 and 2008,6 respectively. Thus, only those articles published in 2014 or later, 55 of 64 in total, could possibly have considered all three time periods of induction. Unfortunately, of those 55 papers published in 2014 or later, almost half (26/55, 47%) focused exclusively on risk during pregnancy, although the risk of acetaminophen exposure for neurodevelopmental injury is probably higher during the peripartum period and during early childhood than in pregnancy.4
Another example of the lack of consideration of a wide range of evidence is the observation that seminal studies were seldom cited in the list of 64 PubMed studies evaluating the role of acetaminophen in neurodevelopmental toxicity (Supplemental Table 4). The first paper describing a connection between acetaminophen and autism, published in 2008,6 was only cited by 27% of the studies. Similarly, the first study showing that acetaminophen is a neurodevelopmental toxin in laboratory animals26 was only cited 24% of the time. In addition, work describing a 2-fold increased risk of autism associated with circumcision,27 a minor medical procedure associated with acetaminophen use, was cited by only 4% of the studies.
Another example of the lack of consideration of a wide range of evidence can be found in studies concluding that no evidence of risk of acetaminophen for neurodevelopment exists (Figure 1). In the past decade, all studies concluding that no evidence of risk of acetaminophen exists limited their conclusions to laboratory animals or to exposure during pregnancy, when risks are most likely the lowest, but possibly not completely absent.4 Importantly, the critically important caveat that the risks of acetaminophen exposure for neurodevelopment during the last hours of pregnancy, during labor and delivery, are apparently extremely high, was never considered in studies concluding that the risks of acetaminophen for neurodevelopment were low during pregnancy.
Mishandling of evidence 3: Irrational criticisms of some evidence
The third way that mishandling of evidence was observed in the literature consisted of irrational criticisms of prior research. This type of mishandling resulted in the rejection or dismissal of evidence, either completely or partially, with irrational or incorrect reasoning. The approach relied not on any valid criticism, but rather on the weight of multiple, invalid and irrational criticisms being levied successively or simultaneously. This type of mishandling affected two out of three papers selected as some of the most compelling “standalone” evidence that acetaminophen is a developmental neurotoxin. As described above in the Methods, three studies—Viberg et al26 in 2013, Schultz et al6 in 2008, and Frisch and Simonsen27 in 2015, present some of the most compelling “standalone” evidence that acetaminophen triggers autism in susceptible babies and children. As described above, the interpretation of the importance of the Viberg et al study and other studies using laboratory animal models has been profoundly affected by the first type of mishandling of evidence described, mishandling of interacting variables. In contrast, interpretation of the importance of the studies by Schultz et al and by Frisch and Simonsen was affected by mishandling with irrational criticism.
Schultz et al6 used a case-controlled online survey and found that acetaminophen exposure concomitant with the MMR vaccination was associated with autism (HR 2.42, CI 1.25–4.69, p = 0.009). Even more striking, the study also observed an association between acetaminophen use any time between 12 and 18 months of age and regressive autism (HR 20.9, CI 1.33–32.9, p = 0.031). As described in the Introduction, this study simultaneously pointed away from the MMR vaccine as a cause of autism and presented for the first time the hypothesis that acetaminophen could be a critical factor triggering autism. However, the study has rarely been cited, and only three studies citing Schultz made statements that could be considered helpful in terms of promoting change in clinical practice or regulatory guidelines (Supplemental Table 5). Several papers citing Schultz et al. rejected that evidence with multiple irrational criticisms. One paper47 dismissed Schultz et al by claiming there were “fatal flaws” regarding sample size and sample bias, although the sample size was large enough to provide statistically significant results and no actual bias that could undermine the conclusions of the study was identified.3,48 Further, two Cochrane reports49,50 dismissed Schultz et al with no explanation other than the note that “Data were obtained via a parent survey; methods and results are questionable.” However, a survey is accepted as a valid approach in modern research.51 Indeed, a subsequent analysis finds that all of the immediate negative responses47 to the Schultz study similarly contained overt errors while lacking valid criticisms.3,48
A perhaps even more haphazard example of “irrational criticisms of prior research” appeared in responses to Frisch and Simonsen.27 In 2015, Frisch and Simonsen27 found male circumcision was strongly associated with infantile autism (HR 2.06, CI 1.36–3.13). This evidence points to acetaminophen, often used in conjunction with male circumcision, as a trigger for autism. Given that Frisch and Simonsen adjusted for several interacting variables related to oxidative stress (Mishandling of evidence 1, above), the study potentially underestimated the association between acetaminophen and autism.2 Further, Frish and Simonsen reported that “data limitations” most likely resulted in underestimations of the actual associations between circumcision and autism. Thus, the association between circumcision and autism was probably stronger than that reported by Frisch and Simonsen.
Despite its compelling nature, only 18 manuscripts are listed in PubMed as citing Frisch and Simonsen, and only one of those makes a statement that would be considered helpful in terms of promoting changes in clinical practice or regulatory guidelines (Supplemental Table 6). For the most part, the evidence from Frisch and Simonsen was irrationally dismissed. In particular, six articles by Morris and various colleagues52,53,54,55,56,57 levied approximately 20 relatively distinct criticisms against Frisch and Simonsen, in various combinations of up to 10 distinct criticisms at a time (Supplemental Table 7). But none of the criticisms were valid (Supplemental Table 7). Some criticisms misunderstood or misrepresented the study, such as the claim that Frisch and Simonsen failed to explain how it was possible that circumcision could be associated with autism.52 However, Frish and Simonsen27 had in fact clearly explained the hypothesis, proposed earlier by Bauer and Kriebel,46 that acetaminophen use during circumcision could trigger autism. Other criticisms involved speculation, such as when Morris et al.54 dismissed Frisch and Simonsen’s conclusions by claiming that the association between circumcision and autism could be explained by undiscovered confounding factors and when Morris and Wiswell57 concluded that “Most likely, both autism spectrum disorder diagnosis and early circumcision reflect parental conscientiousness.” However, they offer no evidence for such claims. Still other criticisms are levied by citing “others” or “critics”52,54,55,56 who disagree with or are implied to disagree with the conclusions of Frisch and Simonsen. However, “appeals to authority” are not valid arguments in scientific reasoning, especially here where the “authorities” cited includes other studies with Morris as a coauthor, an informal blog written by an anonymous source, a magazine article written by a science reporter, and a study that does not actually criticize Frisch and Simonsen in any way (Supplemental Table 7). Taken together, the Morris et al papers’ many invalid criticisms of Frisch and Simonsen amount to an attempt to undermine valid research using a haphazard, scattergun approach relying on volume and repetition of arguments rather than valid scientific reasoning.
The study by Frisch and Simonsen has been validated by other work, which should have undermined unfair criticism. For example, in 2019, a profound association between cord blood acetaminophen metabolites and autism was described by Ji and colleagues,28 providing and independent validation of the enhanced sensitivity of neurodevelopment to acetaminophen at the time of birth that was first suggested by Bauer46 and expected based on pharmacokinetic considerations.4 In addition, a 2020 study by Maini et al. found changes in social behavior associated with circumcised males,58 including dramatic increases in attachment anxiety and attachment avoidance. Approximately 44% of the circumcised males in that study were born prior to 1982 (See Supplemental Table 8), when use of acetaminophen in pediatrics was less common, so the study may have underestimated the neurodevelopmental impact current circumcision practices that do use acetaminophen. Nevertheless, the results obtained by Maini et al. add further support to the observations made by Frisch and Simonsen. But, despite apparent validation, the lack of citations of Frisch and Simonsen’s work in articles discussing the neurodevelopmental impact of acetaminophen indicates that the work conducted by Frisch and Simonsen has been uninfluential in discussions of the role of acetaminophen in the induction of autism.
Discussion
No single problem underlying widespread failure to accept current evidence
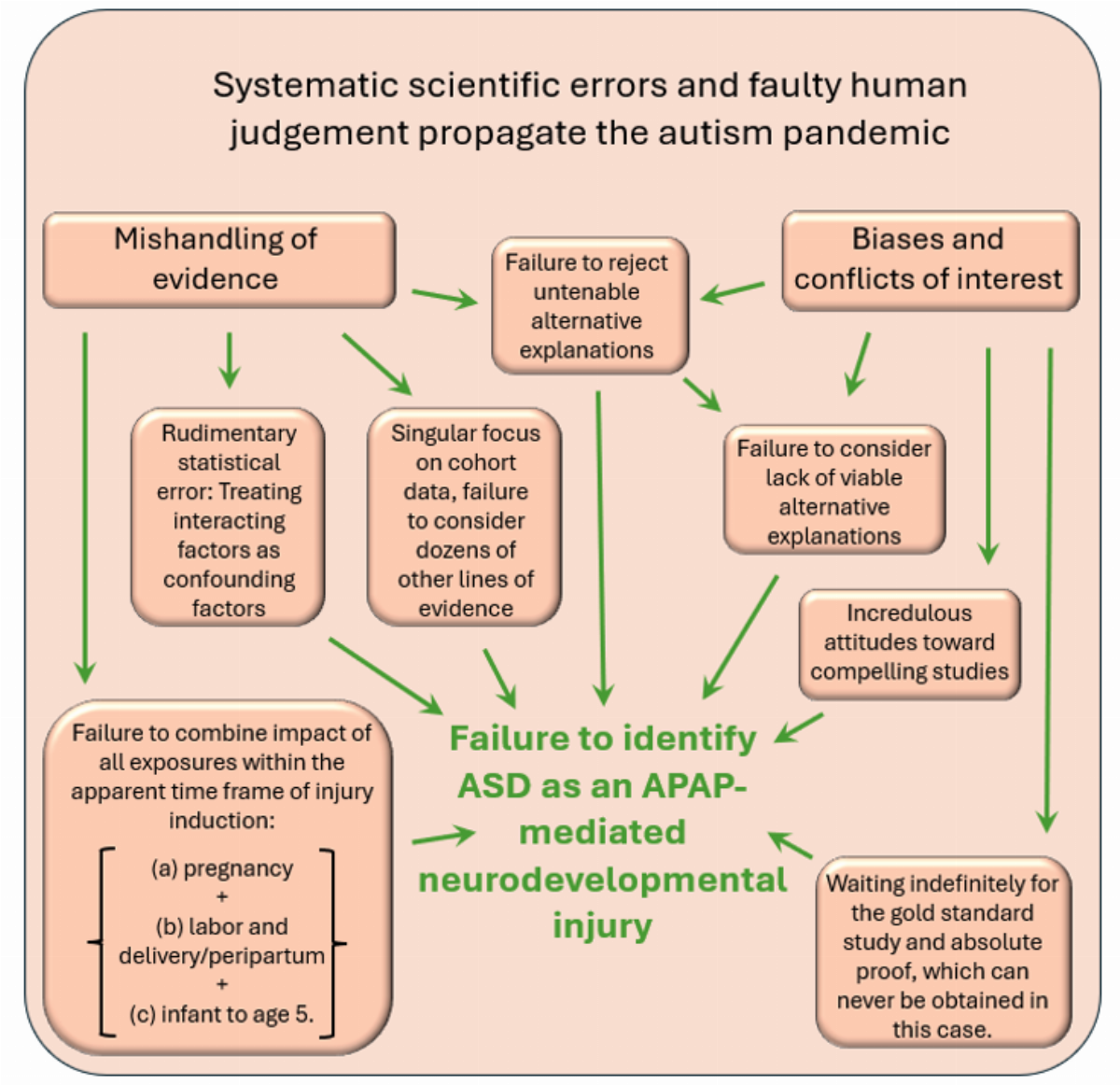
This study used two approaches to identify how evidence related to the acetaminophen mediated induction of autism in susceptible babies and children, and possibly in utero, has been mishandled. One approach surveyed literature discussing the connection between acetaminophen and autism, and the other approach probed the handling of specific lines of evidence related to the connection between acetaminophen and autism. Three errors were identified, each involving a distinct technical or conceptual error in the execution of the science involved: (1) erroneous assumptions underlying statistical analyses, (2) consideration of limited evidence when drawing conclusions, and (3) unfairly criticizing potentially ground-breaking research.
This study shows that the impact of aberrant adjustment for oxidative stress-related variables is very widespread, and has affected the interpretation of many studies. For example, Khan and colleagues30 provide lists of potential confounding factors that were adjusted for in each of a dozen studies published between 2016 and 2020 addressing the association between acetaminophen and autism. In a more recent example, published in 2024, Ahlqvist and colleagues59 adjusted for the presence of more than 25 oxidative stress-related variables, incorrectly concluding that the almost 2-fold increased risk of autism associated with heavy use of acetaminophen during neurodevelopment (HR 1.87 (CI 1.71-2.06), p < 0.001) was entirely due to genetics and a host of other factors, most associated with oxidative stress.
This study also shows that most studies addressing the neurodevelopmental impact of acetaminophen fail to consider evidence from critical periods of development. Conclusive evidence indicates that acetaminophen is a potent neurodevelopmental toxin in the peripartum period, and that neurodevelopmental injury can occur up to the age of about 5, at which time regression into autism becomes rare.4 In addition, adverse neurodevelopmental effects of acetaminophen during pregnancy seem likely, although the sensitive period during pregnancy is not well defined. Importantly, only 15 studies (15/64, 23%) considered information about the neurodevelopmental impact of acetaminophen during pregnancy, the peripartum period, and the postnatal period. This issue is important for two primary reasons. First, focus on only one period of exposure will necessarily exclude significant exposures and diminish the perceived overall impact of acetaminophen on neurodevelopment and the perceived consequences of that impact for society. Second, in terms of changes in clinical practice, physicians that treat women before and during pregnancy (gynecologists and general practitioners) are different than physicians who specialize in the peripartum period (obstetricians), who in turn are different than the physicians who treat children after birth (pediatricians). Thus, when considering changes in clinical practice, it is necessary to consider the entire neurodevelopmental window defined by sensitivity to injury, not subsets of that window defined by current medical practice or other factors. Unfortunately, most studies describing the connection between acetaminophen and autism are limited in their scope.
Study limitations
The present study was not designed to cover every statement regarding acetaminophen and autism made in the peer reviewed literature. Some studies that may address the topic are potentially not listed in PubMed, and others that are listed in PubMed may not contain both autism and acetaminophen in any PubMed search field. However, this approach was considered sufficient to provide an overview of studies which focused on the connection between acetaminophen and autism, with the understanding that not every view expressed in the literature would necessarily be included.
Other limitations of this study include the fact that unfair criticisms of studies were only documented in two cases, and an exhaustive assessment of this type of mishandling of evidence was not performed. Thus, the pervasiveness of this problem is currently unknown. In addition, some types of mishandling of evidence not listed here were found, but not probed in detail. For example, results were sometimes inaccurately described, or described in a misleading way. One study containing this error60 observed more than twice the prevalence of autism in acetaminophen treated children compared to non-treated children (0.69% vs. 0.30%), but concluded that “Intravenous paracetamol given to neonates did not associate with childhood disorders compared with the non-exposed infants during the 5-year follow-up. The previous hypothesis that early paracetamol use causes childhood morbidities was not confirmed.” A possibly more accurate and certainly more informative description of the results would have been that acetaminophen use was associated with more than double the prevalence of autism, but that the study was not sufficiently powered to determine if the association was statistically significant.
Another limitation of this study is that it does not probe the influence of waiting for the “gold standard” of a randomized, controlled trial before any conclusions can be drawn. Some authors in the field recognize that conducting a randomized, controlled trial with acetaminophen use during early neurodevelopment is both infeasible and unethical.61,62,63 Other authors have conducted a controlled trial that spanned the first five years of life,60 but that trial follows a very limited number of children, and it controlled exposures only during a very short time frame. However, other authors suggest that a randomized, controlled trial (RCT) is necessary before any conclusions regarding the role of acetaminophen in the induction of autism can be drawn. For example, in 2025 Coluzzi and colleagues64 stated that “despite some reports on the potential dangers of neurodevelopment impairment in susceptible babies and children exposed to acetaminophen, especially during pregnancy or in the early post-partum period,4 there is no evidence from RCTs to support or refute its use in pediatric age.” The article cited here by Coluzzi and colleagues, a paper that includes coauthors RA, JPJ, ZK, LW, and WP,4 describes 22 lines of evidence pointing to the conclusion “without reasonable doubt and with no evidence to the contrary that exposure of susceptible babies and children to acetaminophen induces many, if not most, cases of autism”. To characterize that paper as describing “potential dangers” could be considered misleading. More importantly, waiting for a randomized, controlled trial before drawing any clinically relevant conclusions is self-defeating and constitutes a profound error given that such studies are not feasible or ethical to conduct in an effective manner. The influence of this error may require studies aimed at assessment of attitudes among recognized experts in the field, and no attempt was made to quantify that influence in the present study.
Another limitation of this study is that it does not systematically probe economic or financial factors that might have an adverse impact on the science related to acetaminophen and autism. For example, the role of industry interference with the scientific process, long known to be a significant inhibitor to progress in the field of science,65,66,67,68,69,70,71,72 was not probed systematically in this study. In the course of conducting this review, only one manuscript stood out as clearly fitting the criteria of an industry-based attempt to obfuscate the relationship between autism and acetaminophen established by science. That industry-associated study,73 published in 2025, is the only one to conclude that “strong evidence of no adverse effects (of acetaminophen on neurodevelopment)” exists (Figure 1). This report contains a plethora of errors that are obvious (See footnotes on Supplemental Table 2), and it is hoped that the report will have little impact on the field, possibly with the exception of bringing more attention to this vitally important subject area. However, the “industry playbook” contains much more sophisticated tools aimed at obfuscating and impeding science, and it remains to be seen which of these will be or already has been deployed. For example, experiments can be designed with the goal of producing negative results. In a possible example of this approach, one measure of acetaminophen-mediated damage to adult mouse brains following a single dose of acetaminophen was assessed and found to be negative in a 2025 study,74 despite the fact that older studies26,75 had already demonstrated that more than one dose of acetaminophen in neonatal mice, not older mice, is required for acetaminophen-mediated neurodevelopmental brain injury to occur. However, systematic evaluation of intentional misdirection or misinformation in science was not the goal of this study, and awaits further investigation.
Another limitation to this study is that investigator biases and conflicts of interest could not be readily assessed. Evidence for the influence of bias in science is apparent throughout the scientific literature. For example, scientists are averse to certainty,76,77,78 and may embrace uncertainty to the point of delaying necessary changes in policy.76 Further, scientists may have conflicts of interest when it comes to drawing firm conclusions. As pointed out by O’Ryan and colleagues79 in their assessment of current problems in academic research, “Avoidable waste in medical research is fuelled by scientists pressed for funding, who consistently conclude more research (and funds) are needed”. This viewpoint is certainly supported here, with (40/64, 63%) of all studies calling for more research. In addition, consensus bias, confirmation bias, and emotional compromise are present and may affect biomedical researchers and clinicians who have long overlooked the contribution of acetaminophen to neurodevelopmental problems (Reviewed in a preprint by Jones et al.80) However, again, this issue was not addressed in the present study, and awaits further investigation.
Another limitation of this study is that it does not probe some problems found in the literature related to medical considerations regarding the use of acetaminophen during neurodevelopment. For example, clinical recommendations were sometimes made without considering either (a) the rights of patients to be informed of available information, or (b) the cost-to-benefit ratio of acetaminophen use during neurodevelopment. The latter error is of particular interest given that the use of acetaminophen during neurodevelopment has no proven long-term benefits. For example, de Fays and colleagues81 conclude that “Care should be taken to avoid raising poorly founded concerns among pregnant females because of the risk of switching to other analgesic/antipyretic drugs with less favourable risk profile (e.g. nonsteroidal anti-inflammatory drugs).” In this case, the authors’ conclusions were affected by multiple errors in mishandling of evidence, including both adjustment for interacting variables and consideration of limited evidence, documented in this study. In addition, the authors are potentially suggesting that patients should not be informed of risks because they might do something even riskier, an argument which is not likely supported by current ethical guidelines in medicine. While systematic documentation of issues regarding inappropriate clinical recommendations is potentially important, such documentation is beyond the scope of this study.
Conclusions
This systematic review of the literature suggests that several factors contribute to years of failure to halt the ongoing adverse impact of acetaminophen on neurodevelopment. Mishandling and misinterpretation of data are pervasive, particularly errors involving statistical analysis, limiting consideration of acetaminophen-mediated neurodevelopmental injury to some fraction of the total window of sensitivity to injury, and considering evidence from limited fields of research when drawing conclusions. Unfair criticisms of some studies also apparently play a role in the problem. The interpretation of potentially groundbreaking studies has suffered from more than one type of mishandling, possibly representing crucial “forks in the road” that were missed, impeding progress in the field. Although industry-based activity aimed at obfuscating and impeding scientific progress has historically been a problem, published evidence suggests that such activity may not be problematic at the present time with regards to the neurodevelopmental impact of acetaminophen.
Given the limited number of studies that have addressed the connection between acetaminophen and autism (ASD), and given the fundamental nature of pervasive errors in the field, it is apparent that modern science has not been applied to this issue in a vigorous and reasonable manner. At the same time, available evidence is already more than sufficient to establish a causal relationship between acetaminophen and autism, and resolution of the problem need not wait on additional studies. It is hoped that a tipping point will soon be reached, in which stakeholders critically evaluate all available evidence and, as a result, implement changes in regulation and clinical practice, ending more than a century of acetaminophen-mediated neurodevelopmental injury.
Disclosures, Funding & Conflicts of Interest
Acknowledgements: The authors wish to thank Kathryn J. Reissner, Susan Poulton, and John Poulton for invaluable insight and discussion, and thank Spencer Sharpe for assistance with logistics. The authors also thank Vishnu Patel, Caitlin Travers, and Lauren Piper for participation in a panel discussion germane to the study design, and the Interlibrary Borrowing staff at the University of North Carolina, Chapel Hill Library for their extensive work that was vital to the conduct of this study. The authors also thank Vishnu Patel and Caitlin Travers for assistance with the systematic review and for careful reading of the manuscript. In addition, the authors thank Zoie E. Holzknecht for careful reading of the manuscript.
Author Contributions
Coauthors RA, RRB and WP conceptualized the study.
Coauthors PTC, RA, RRB, and WP contributed to study design and executed that design, including data collection and analysis.
Coauthors PTC, JPJ III, ZK, LW, and RRB critically reviewed and revised the manuscript for important intellectual content.
All authors approved the final manuscript as submitted.
Conflict of Interest Disclosures: The authors have no conflicts of interest relevant to this article to disclose.
Funding: This work was funded in part by generous donations to WPLab, Inc., a non-profit corporation based in Durham, North Carolina.
References
Patel E, Jones Iii JP, 3rd, Bono-Lunn D, Kuchibhatla M, Palkar A, Cendejas Hernandez J, et al. The safety of pediatric use of paracetamol (acetaminophen): a narrative review of direct and indirect evidence. Minerva pediatrics. 2022;74(6):774-88. Epub 2022/07/14. doi: 10.23736/s2724-5276.22.06932-4. PubMed PMID: 35822581.
Jones JP, 3rd, Williamson L, Konsoula Z, Anderson R, Reissner KJ, Parker W. Evaluating the Role of Susceptibility Inducing Cofactors and of Acetaminophen in the Etiology of Autism Spectrum Disorder. Life (Basel, Switzerland). 2024;14(8). Epub 2024/08/31. doi: 10.3390/life14080918. PubMed PMID: 39202661; PubMed Central PMCID: PMCPMC11355895.
Zhao L, Jones J, Anderson L, Konsoula Z, Nevison C, Reissner K, et al. Acetaminophen causes neurodevelopmental injury in susceptible babies and children: no valid rationale for controversy. Clinical and experimental pediatrics. 2023. Epub 2023/06/16. doi: 10.3345/cep.2022.01319. PubMed PMID: 37321575.
Parker W, Anderson LG, Jones JP, Anderson R, Williamson L, Bono-Lunn D, et al. The Dangers of Acetaminophen for Neurodevelopment Outweigh Scant Evidence for Long-Term Benefits. Children. 2024;11(1):44. PubMed PMID: doi:10.3390/children11010044.
Parker W, Hornik CD, Bilbo S, Holzknecht ZE, Gentry L, Rao R, et al. The role of oxidative stress, inflammation and acetaminophen exposure from birth to early childhood in the induction of autism. J Int Med Res. 2017;45(2):407-38.
Schultz ST, Klonoff-Cohen HS, Wingard DL, Akshoomoff NA, Macera CA, Ji M. Acetaminophen (paracetamol) use, measles-mumps-rubella vaccination, and autistic disorder. The results of a parent survey. Autism. 2008;12(3):293-307.
Good P. Did acetaminophen provoke the autism epidemic? Alternative Medicine Review. 2009;14(4):364-72.
Matsuishi T, Shiotsuki Y, Yoshimura K, Shoji H, Imuta F, Yamashita F. High prevalence of infantile autism in Kurume City, Japan. J Child Neurol. 1987;2(4):268-71. Epub 1987/10/01. doi: 10.1177/088307388700200406. PubMed PMID: 3498744.
Alberti A, Pirrone P, Elia M, Waring RH, Romano C. Sulphation deficit in "low-functioning" autistic children: a pilot study. Biol Psychiatry. 1999;46(3):420-4. Epub 1999/08/06. doi: 10.1016/s0006-3223(98)00337-0. PubMed PMID: 10435209.
Prescott L. The Metabolism of Paracetamol. Acetaminophen (Paracetamol) A Critical Bibliographic Review. Abingdon, UK: Taylor & Francis; 1996. p. 82.
Anvik JO. Acetaminophen toxicosis in a cat. The Canadian veterinary journal = La revue veterinaire canadienne. 1984;25(12):445-7. Epub 1984/12/01. PubMed PMID: 17422485; PubMed Central PMCID: PMCPMC1790690.
Savides MC, Oehme FW, Nash SL, Leipold HW. The toxicity and biotransformation of single doses of acetaminophen in dogs and cats. Toxicol Appl Pharmacol. 1984;74(1):26-34. Epub 1984/06/15. doi: 10.1016/0041-008x(84)90266-7. PubMed PMID: 6729821.
St Omer VV, McKnight ED, 3rd. Acetylcysteine for treatment of acetaminophen toxicosis in the cat. J Am Vet Med Assoc. 1980;176(9):911-3. Epub 1980/05/01. PubMed PMID: 7400022.
Miller RP, Roberts RJ, Fischer LJ. Acetaminophen elimination kinetics in neonates, children, and adults. Clin Pharmacol Ther. 1976;19(3):284-94. Epub 1976/03/01. doi: 10.1002/cpt1976193284. PubMed PMID: 1261167.
Levy G, Khanna NN, Soda DM, Tsuzuki O, Stern L. Pharmacokinetics of acetaminophen in the human neonate: formation of acetaminophen glucuronide and sulfate in relation to plasma bilirubin concentration and D-glucaric acid excretion. Pediatrics. 1975;55(6):818-25. Epub 1975/06/01. PubMed PMID: 1134883.
Cendejas-Hernandez J, Sarafian J, Lawton V, Palkar A, Anderson L, Lariviere V, et al. Paracetamol (Acetaminophen) Use in Infants and Children was Never Shown to be Safe for Neurodevelopment: A Systematic Review with Citation Tracking. . Eur J Pediatr. 2022;181:1835-57. doi: 10.1007/s00431-022-04407-w.
Green MD, Shires TK, Fischer LJ. Hepatotoxicity of acetaminophen in neonatal and young rats. I. Age-related changes in susceptibility. Toxicol Appl Pharmacol. 1984;74(1):116-24. Epub 1984/06/15. doi: 10.1016/0041-008x(84)90277-1. PubMed PMID: 6729816.
Freed GL, Clark SJ, Butchart AT, Singer DC, Davis MM. Parental vaccine safety concerns in 2009. Pediatrics. 2010;125(4):654-9. Epub 2010/03/03. doi: 10.1542/peds.2009-1962. PubMed PMID: 20194286.
Bazzano A, Zeldin A, Schuster E, Barrett C, Lehrer D. Vaccine-related beliefs and practices of parents of children with autism spectrum disorders. Am J Intellect Dev Disabil. 2012;117(3):233-42. Epub 2012/06/22. doi: 10.1352/1944-7558-117.3.233. PubMed PMID: 22716265.
Fischbach RL, Harris MJ, Ballan MS, Fischbach GD, Link BG. Is there concordance in attitudes and beliefs between parents and scientists about autism spectrum disorder? Autism. 2016;20(3):353-63. Epub 2015/05/28. doi: 10.1177/1362361315585310. PubMed PMID: 26014839.
Bonsu NEM, Mire SS, Sahni LC, Berry LN, Dowell LR, Minard CG, et al. Understanding Vaccine Hesitancy Among Parents of Children With Autism Spectrum Disorder and Parents of Children With Non-Autism Developmental Delays. J Child Neurol. 2021;36(10):911-8. Epub 2021/05/29. doi: 10.1177/08830738211000505. PubMed PMID: 34048284; PubMed Central PMCID: PMCPMC8440329.
Rimland B. The autism increase: research needed on the vaccine connection. Autism Research Review International. 2000.
Goldberg D. MMR, autism, and adam. BMJ. 2000;320(7231):389. Epub 2000/02/05. PubMed PMID: 10657358; PubMed Central PMCID: PMCPMC1127168.
Schultz S. Understanding Autism: My Quest for Nathan: Schultz Publishing LLC; 2013. 92 p.
Werner E, Dawson G. Validation of the phenomenon of autistic regression using home videotapes. Arch Gen Psychiatry. 2005;62(8):889-95. Epub 2005/08/03. doi: 10.1001/archpsyc.62.8.889. PubMed PMID: 16061766.
Viberg H, Eriksson P, Gordh T, Fredriksson A. Paracetamol (Acetaminophen) Administration During Neonatal Brain Development Affects Cognitive Function and Alters Its Analgesic and Anxiolytic Response in Adult Male Mice. Toxicol Sci. 2013;138(1):139-47. doi: 10.1093/toxsci/kft329.
Frisch M, Simonsen J. Ritual circumcision and risk of autism spectrum disorder in 0- to 9-year-old boys: national cohort study in Denmark. J R Soc Med. 2015;108(7):266-79. doi: 10.1177/0141076814565942. PubMed PMID: PMC4530408.
Ji Y, Azuine RE, Zhang Y, Hou W, Hong X, Wang G, et al. Association of Cord Plasma Biomarkers of In Utero Acetaminophen Exposure With Risk of Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder in Childhood. JAMA Psychiatry. 2020;77(2):180-9. Epub 2019/10/31. doi: 10.1001/jamapsychiatry.2019.3259. PubMed PMID: 31664451; PubMed Central PMCID: PMCPMC6822099.
Brandlistuen RE, Ystrom E, Nulman I, Koren G, Nordeng H. Prenatal paracetamol exposure and child neurodevelopment: a sibling-controlled cohort study. Int J Epidemiol. 2013;42(6):1702-13.
Khan FY, Kabiraj G, Ahmed MA, Adam M, Mannuru SP, Ramesh V, et al. A Systematic Review of the Link Between Autism Spectrum Disorder and Acetaminophen: A Mystery to Resolve. Cureus. 2022;14(7):e26995. doi: 10.7759/cureus.26995.
Blecharz-Klin K, Wawer A, Jawna-Zboińska K, Pyrzanowska J, Piechal A, Mirowska-Guzel D, et al. Early paracetamol exposure decreases brain-derived neurotrophic factor (BDNF) in striatum and affects social behaviour and exploration in rats. Pharmacol Biochem Behav. 2018;168:25-32. Epub 2018/03/17. doi: 10.1016/j.pbb.2018.03.004. PubMed PMID: 29545027.
Palta P, Szanton SL, Semba RD, Thorpe RJ, Varadhan R, Fried LP. Financial strain is associated with increased oxidative stress levels: the Women's Health and Aging Studies. Geriatric nursing (New York, NY). 2015;36(2 Suppl):S33-7. Epub 2015/03/19. doi: 10.1016/j.gerinurse.2015.02.020. PubMed PMID: 25784083; PubMed Central PMCID: PMCPMC6053071.
Eick SM, Barrett ES, van 't Erve TJ, Nguyen RHN, Bush NR, Milne G, et al. Association between prenatal psychological stress and oxidative stress during pregnancy. Paediatr Perinat Epidemiol. 2018;32(4):318-26. Epub 03/30. doi: 10.1111/ppe.12465. PubMed PMID: 29603338.
Skrabalova J, Drastichova Z, Novotny J. Morphine as a Potential Oxidative Stress-Causing Agent. Mini-reviews in organic chemistry. 2013;10(4):367-72. Epub 2014/01/01. doi: 10.2174/1570193x113106660031. PubMed PMID: 24376392; PubMed Central PMCID: PMCPMC3871421.
Kalghatgi S, Spina CS, Costello JC, Liesa M, Morones-Ramirez JR, Slomovic S, et al. Bactericidal antibiotics induce mitochondrial dysfunction and oxidative damage in Mammalian cells. Science translational medicine. 2013;5(192):192ra85. Epub 2013/07/05. doi: 10.1126/scitranslmed.3006055. PubMed PMID: 23825301; PubMed Central PMCID: PMCPMC3760005.
Moller P, Wallin H, Knudsen LE. Oxidative stress associated with exercise, psychological stress and life-style factors. Chem-Biol Interact. 1996;102(1):17-36.
Lean SC, Jones RL, Roberts SA, Heazell AEP. A prospective cohort study providing insights for markers of adverse pregnancy outcome in older mothers. BMC pregnancy and childbirth. 2021;21(1):706. Epub 2021/10/22. doi: 10.1186/s12884-021-04178-6. PubMed PMID: 34670515; PubMed Central PMCID: PMCPMC8527686.
Marseglia L, Manti S, D'Angelo G, Nicotera A, Parisi E, Di Rosa G, et al. Oxidative stress in obesity: a critical component in human diseases. Int J Mol Sci. 2014;16(1):378-400. Epub 2014/12/31. doi: 10.3390/ijms16010378. PubMed PMID: 25548896; PubMed Central PMCID: PMCPMC4307252.
Krishnamurthy HK, Rajavelu I, Pereira M, Jayaraman V, Krishna K, Wang T, et al. Inside the genome: understanding genetic influences on oxidative stress. Front Genet. 2024;15:1397352. Epub 2024/07/10. doi: 10.3389/fgene.2024.1397352. PubMed PMID: 38983269; PubMed Central PMCID: PMCPMC11231378.
Forsberg L, de Faire U, Morgenstern R. Oxidative stress, human genetic variation, and disease. Arch Biochem Biophys. 2001;389(1):84-93. Epub 2001/05/24. doi: 10.1006/abbi.2001.2295. PubMed PMID: 11370676.
Shelton RC, Claiborne J, Sidoryk-Wegrzynowicz M, Reddy R, Aschner M, Lewis DA, et al. Altered expression of genes involved in inflammation and apoptosis in frontal cortex in major depression. Mol Psychiatry. 2011;16(7):751-62. doi: 10.1038/mp.2010.52. PubMed PMID: PMC2928407.
Berk M, Williams LJ, Jacka FN, O'Neil A, Pasco JA, Moylan S, et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC medicine. 2013;11:200. Epub 2013/11/16. doi: 10.1186/1741-7015-11-200. PubMed PMID: 24228900; PubMed Central PMCID: PMCPMC3846682.
Salim S. Oxidative Stress and the Central Nervous System. J Pharmacol Exp Ther. 2017;360(1):201-5. Epub 2016/10/19. doi: 10.1124/jpet.116.237503. PubMed PMID: 27754930; PubMed Central PMCID: PMCPMC5193071.
Foo J, Bellot G, Pervaiz S, Alonso S. Mitochondria-mediated oxidative stress during viral infection. Trends Microbiol. 2022;30(7):679-92. Epub 2022/01/23. doi: 10.1016/j.tim.2021.12.011. PubMed PMID: 35063304.
Milhelm Z, Zanoaga O, Pop L, Iovita A, Chiroi P, Harangus A, et al. Evaluation of oxidative stress biomarkers for differentiating bacterial and viral infections: a comparative study of glutathione disulfide (GSSG) and reduced glutathione (GSH). Medicine and pharmacy reports. 2025;98(1):46-53. Epub 2025/02/14. doi: 10.15386/mpr-2821. PubMed PMID: 39949919; PubMed Central PMCID: PMCPMC11817587.
Bauer A, Kriebel D. Prenatal and perinatal analgesic exposure and autism: an ecological link. Environmental Health. 2013;12(1):41. PubMed PMID: doi:10.1186/1476-069X-12-41.
Cox AR, McDowell S. A response to the article on the association between paracetamol/acetaminophen: use and autism by Stephen T. Schultz. Autism. 2009;13(1):123-4; author reply 4-5. Epub 2009/01/30. doi: 10.1177/1362361308101816. PubMed PMID: 19176580.
Schultz ST. Response to the Letter by Cox and McDowell: Association of Paracetamol/Acetaminophen Use and Autism. Autism. 2009;13(1):124-5. doi: 10.1177/13623613090130010802.
Di Pietrantonj C, Rivetti A, Marchione P, Debalini MG, Demicheli V. Vaccines for measles, mumps, rubella, and varicella in children. Cochrane Database Syst Rev. 2021;(11). doi: 10.1002/14651858.CD004407.pub5. PubMed PMID: CD004407.
Di Pietrantonj C, Rivetti A, Marchione P, Debalini MG, Demicheli V. Vaccines for measles, mumps, rubella, and varicella in children. Cochrane Database Syst Rev. 2020;4(4):Cd004407. Epub 2020/04/21. doi: 10.1002/14651858.CD004407.pub4. PubMed PMID: 32309885; PubMed Central PMCID: PMCPMC7169657 Marchione: none known Maria Grazia Debalini: none known Vittorio Demicheli: none known.
Tenny S, Kerndt CC, Hoffman MR. Case Control Studies. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC.; 2025.
Morris BJ, Moreton S, Krieger JN, Klausner JD. Infant Circumcision for Sexually Transmitted Infection Risk Reduction Globally. Global health, science and practice. 2022;10(4). Epub 2022/08/31. doi: 10.9745/ghsp-d-21-00811. PubMed PMID: 36041835; PubMed Central PMCID: PMCPMC9426975.
Morris BJ, Katelaris A, Blumenthal NJ, Hajoona M, Sheen AC, Schrieber L, et al. Evidence-based circumcision policy for Australia. Journal of men's health. 2022;18(6). Epub 2022/08/30. doi: 10.31083/j.jomh1806132. PubMed PMID: 36034719; PubMed Central PMCID: PMCPMC9409339.
Morris BJ, Moreton S, Bailis SA, Cox G, Krieger JN. Critical evaluation of contrasting evidence on whether male circumcision has adverse psychological effects: A systematic review. Journal of evidence-based medicine. 2022;15(2):123-35. Epub 2022/07/06. doi: 10.1111/jebm.12482. PubMed PMID: 35785439; PubMed Central PMCID: PMCPMC9540570.
Morris BJ, Moreton S, Krieger JN. Critical evaluation of arguments opposing male circumcision: A systematic review. Journal of evidence-based medicine. 2019;12(4):263-90. Epub 2019/09/10. doi: 10.1111/jebm.12361. PubMed PMID: 31496128; PubMed Central PMCID: PMCPMC6899915.
Morris BJ, Krieger JN, Klausner JD. CDC's Male Circumcision Recommendations Represent a Key Public Health Measure. Global health, science and practice. 2017;5(1):15-27. Epub 2017/03/30. doi: 10.9745/ghsp-d-16-00390. PubMed PMID: 28351877; PubMed Central PMCID: PMCPMC5478224.
Morris BJ, Wiswell TE. 'Circumcision pain' unlikely to cause autism. J R Soc Med. 2015;108(8):297. Epub 2015/08/14. doi: 10.1177/0141076815590404. PubMed PMID: 26268916; PubMed Central PMCID: PMCPMC4535438.
Miani A, Di Bernardo GA, Højgaard AD, Earp BD, Zak PJ, Landau AM, et al. Neonatal male circumcision is associated with altered adult socio-affective processing. Heliyon. 2020;6(11):e05566. Epub 2020/12/11. doi: 10.1016/j.heliyon.2020.e05566. PubMed PMID: 33299934; PubMed Central PMCID: PMCPMC7702013.
Ahlqvist VH, Sjöqvist H, Dalman C, Karlsson H, Stephansson O, Johansson S, et al. Acetaminophen Use During Pregnancy and Children's Risk of Autism, ADHD, and Intellectual Disability. Jama. 2024;331(14):1205-14. Epub 2024/04/09. doi: 10.1001/jama.2024.3172. PubMed PMID: 38592388; PubMed Central PMCID: PMCPMC11004836.
Juujärvi S, Saarela T, Pokka T, Hallman M, Aikio O. Intravenous paracetamol for neonates: long-term diseases not escalated during 5 years of follow-up. Archives of disease in childhood Fetal and neonatal edition. 2021;106(2):178-83. Epub 2020/09/19. doi: 10.1136/archdischild-2020-319069. PubMed PMID: 32943529.
Qubty W, Gelfand AA. The Link Between Infantile Colic and Migraine. Current pain and headache reports. 2016;20(5):31. Epub 2016/04/04. doi: 10.1007/s11916-016-0558-8. PubMed PMID: 27038970.
Liew Z, Ritz B, Virk J, Olsen J. Maternal use of acetaminophen during pregnancy and risk of autism spectrum disorders in childhood: A Danish national birth cohort study. Autism research : official journal of the International Society for Autism Research. 2016;9(9):951-8. Epub 2015/12/22. doi: 10.1002/aur.1591. PubMed PMID: 26688372.
Liew Z, Ernst A. Intrauterine Exposure to Acetaminophen and Adverse Developmental Outcomes: Epidemiological Findings and Methodological Issues. Current environmental health reports. 2021;8(1):23-33. Epub 2021/01/06. doi: 10.1007/s40572-020-00301-5. PubMed PMID: 33398668.
Coluzzi F, Di Stefano G, Scerpa MS, Rocco M, Di Nardo G, Innocenti A, et al. The Challenge of Managing Neuropathic Pain in Children and Adolescents with Cancer. Cancers. 2025;17(3). Epub 2025/02/13. doi: 10.3390/cancers17030460. PubMed PMID: 39941827; PubMed Central PMCID: PMCPMC11816330.
Lexchin J, Bero LA, Djulbegovic B, Clark O. Pharmaceutical industry sponsorship and research outcome and quality: systematic review. BMJ. 2003;326(7400):1167-70. Epub 2003/05/31. doi: 10.1136/bmj.326.7400.1167. PubMed PMID: 12775614; PubMed Central PMCID: PMCPMC156458.
Bero LA. Tobacco industry manipulation of research. Public health reports (Washington, DC : 1974). 2005;120(2):200-8. Epub 2005/04/22. doi: 10.1177/003335490512000215. PubMed PMID: 15842123; PubMed Central PMCID: PMCPMC1497700.
Fabbri A, Holland TJ, Bero LA. Food industry sponsorship of academic research: investigating commercial bias in the research agenda. Public health nutrition. 2018;21(18):3422-30. Epub 2018/08/31. doi: 10.1017/s1368980018002100. PubMed PMID: 30157979; PubMed Central PMCID: PMCPMC10260999.
Whitstock M. Manufacturing the truth: From designing clinical trials to publishing trial data. Indian journal of medical ethics. 2018;3(2):152-62. Epub 2017/12/19. doi: 10.20529/ijme.2017.096. PubMed PMID: 29251608.
Gupta R, Chernesky J, Lembke A, Michaels D, Tomori C, Greene JA, et al. The opioid industry's use of scientific evidence to advance claims about prescription opioid safety and effectiveness. Health affairs scholar. 2024;2(10):qxae119. Epub 2024/10/25. doi: 10.1093/haschl/qxae119. PubMed PMID: 39450313; PubMed Central PMCID: PMCPMC11500661.
Legg T, Hatchard J, Gilmore AB. The Science for Profit Model-How and why corporations influence science and the use of science in policy and practice. PLoS One. 2021;16(6):e0253272. Epub 2021/06/24. doi: 10.1371/journal.pone.0253272. PubMed PMID: 34161371; PubMed Central PMCID: PMCPMC8221522.
Tran TH, Steffen JE, Clancy KM, Bird T, Egilman DS. Talc, Asbestos, and Epidemiology: Corporate Influence and Scientific Incognizance. Epidemiology. 2019;30(6):783-8. Epub 2019/08/31. doi: 10.1097/ede.0000000000001091. PubMed PMID: 31469695; PubMed Central PMCID: PMCPMC6784763.
Brownell KD, Warner KE. The perils of ignoring history: Big Tobacco played dirty and millions died. How similar is Big Food? Milbank Q. 2009;87(1):259-94. Epub 2009/03/21. doi: 10.1111/j.1468-0009.2009.00555.x. PubMed PMID: 19298423; PubMed Central PMCID: PMCPMC2879177.
Kougias DG, Atillasoy E, Southall MD, Scialli AR, Ejaz S, Chu C, et al. A quantitative weight-of-evidence review of preclinical studies examining the potential developmental neurotoxicity of acetaminophen. Crit Rev Toxicol. 2025:1-55. Epub 2025/02/21. doi: 10.1080/10408444.2024.2442344. PubMed PMID: 39982125.
Ali NA, Kennon-McGill S, Parker LD, James LP, Fantegrossi WE, McGill MR. NAPQI is absent in the mouse brain after sub-hepatotoxic and hepatotoxic doses of acetaminophen. Toxicol Sci. 2025;205(2):274-8. Epub 2025/03/11. doi: 10.1093/toxsci/kfaf034. PubMed PMID: 40065514; PubMed Central PMCID: PMCPMC12118958.
Philippot G, Gordh T, Fredriksson A, Viberg H. Adult neurobehavioral alterations in male and female mice following developmental exposure to paracetamol (acetaminophen): characterization of a critical period. J Appl Toxicol. 2017;37(10):1174-81. Epub 2017/04/28. doi: 10.1002/jat.3473. PubMed PMID: 28448685.
Freudenburg WR, Gramling R, Davidson DJ. Scientific Certainty Argumentation Methods (SCAMs): Science and the Politics of Doubt. Sociological Inquiry. 2008;78(1):2-38. doi: https://doi.org/10.1111/j.1475-682X.2008.00219.x.
Clegg JW. Uncertainty as a fundamental scientific value. Integrative psychological & behavioral science. 2010;44(3):245-51. Epub 2010/06/24. doi: 10.1007/s12124-010-9135-6. PubMed PMID: 20571939.
Castillo M. The uncertainty of science and the science of uncertainty. AJNR American journal of neuroradiology. 2010;31(10):1767-8. Epub 2010/04/24. doi: 10.3174/ajnr.A2106. PubMed PMID: 20413608; PubMed Central PMCID: PMCPMC7964029.
O’Ryan ML, Saxena S, Baum F. Time for a revolution in academic medicine? BMJ. 2024;387:q2508. doi: 10.1136/bmj.q2508.
Jones J, Konsoula Z, Williamson L, Anderson R, Meza-Keuthen S, Parker W. Three Mandatory Doses of Acetaminophen During the First Months of Life with the MenB Vaccine: A Protocol for the Induction of Autism Spectrum Disorder in Susceptible Individuals. Preprints: Preprints; 2025.
de Fays L, Van Malderen K, De Smet K, Sawchik J, Verlinden V, Hamdani J, et al. Use of paracetamol during pregnancy and child neurological development. Dev Med Child Neurol. 2015;57(8):718-24. Epub 2015/04/09. doi: 10.1111/dmcn.12745. PubMed PMID: 25851072.
