Abstract
Excess mortality has been observed in several countries since 2021 and has not yet been explained. The aim of this study was to determine whether the age-adjusted mortality rates of non-COVID-19 deaths differed between those who had received one, two, three or four doses compared with the unvaccinated. Data were obtained from the Office for National Statistics of England and categorized by age groups and vaccinations status (unvaccinated or 1 - 4 doses, given at least 21 days previously). Rates among the unvaccinated were used as a benchmark, assuming that COVID-19 vaccination should have no positive or negative effect on the age-adjusted non-COVID-19 mortality rate. The age-adjusted non-COVID-19 mortality rate was higher in all age groups who have received dose 1, but mainly in the elderly. The age-adjusted non-COVID-19 mortality rate also peaked in all those who have received dose 2, mainly in the elderly. Interestingly, age-adjusted non-COVID-19 mortality has a tendency to peak across age groups following the age-dependent timing of vaccination campaigns, both in the first and second vaccination rounds. A fourth finding was the substantially higher age-adjusted non-COVID-19 mortality rates in the 18 – 39 age group among those who had received dose 4. Relevant comorbidities among the vaccinated population may explain the differences (healthy non-vaccinee bias), but these data were not available. Although a causal relationship between excess mortality and vaccination against COVID-19 cannot be established, a higher age-adjusted non-COVID-19 mortality rate among the COVID-19 vaccinated in several age groups was found, that, together with vaccination timing associated mortality peaks require further research.
Keywords: COVID-19 vaccination; excess mortality; non-COVID-19 deaths; age-adjusted mortality rate; England
Affiliations:
Günter Kampf, MD, University Medicine Greifswald, Ferdinand-Sauerbruch-Strasse, 17475 Greifswald, Germany
Maarten Fornerod, MSc, Department of Cell Biology, Erasmus Medical Center, Dr. Molewaterplein 40, 3000 DR Rotterdam, The Netherlands
Correspondence:
Introduction
Since 2021, excess mortality has increased and remains high in several countries.1,2 In Germany, excess deaths reached 34,000 in 2021 and 66,000 in 2022.3 This increase was unexpected.4 It was speculated that an inadequate vaccination level might be the cause.4 A further analysis showed that excess mortality in Germany was positively correlated with COVID-19 infection in 2020. However, a significant positive correlation was observed between the increase in excess mortality and the COVID-19 vaccination rates of the 16 German federal states in 2021 and 2022.5 In Cyprus, one study reported a lack of association between vaccination rates and excess mortality,6 whereas another study described that excess mortality increased and was particularly high in 2021 and 2022.7 Economidou et al. raised serious concerns about the potential impact of the COVID-19 vaccination campaign and other causes of mortality.7 In contrast, in Israel, a cohort of the COVID-19 vaccinated population showed a similar all-cause mortality rate in 2021 compared with the average mortality rate between 2017 and 2019, suggesting no effect of the COVID-19 vaccines on non-COVID-19 mortality, although no distinction was made between the doses of vaccine given.8
Excess mortality is often described as a finding that occurs despite high vaccination coverage,9 suggesting that the vaccination itself is only expected to reduce overall mortality. Faust et al. reported that between January 2020 and July 2022 excess mortality and the number of new COVID-19 cases were decoupled,10 suggesting that causes other than COVID-19 may explain the excess mortality.
In 2021, the possible association between vaccination and excess deaths has been raised,11 but the hypothesis that COVID-19 vaccines might kill some of the recipients was strongly rejected,12 although later in 2021 it was reported that vaccine-associated deaths occur with all major COVID-19 vaccines.13 In June 2023, the German Federal Minister of Health, Karl Lauterbach, was asked in the parliament whether the excess mortality could be explained by the COVID-19 vaccines. He clearly stated that there was no evidence that the excess mortality could be caused by the vaccinations administered, that there was no evidence for this and it was not medically plausible.14
The Office for National Statistics of England publishes the number of deaths and the age-adjusted mortality rates by vaccination status and distinguishes between COVID-19-related deaths and non-COVID-19 deaths. The aim of this study was to find out whether the age-adjusted mortality rates of non-COVID-19 deaths differed between those who had received one, two, three or four doses and those who had not been unvaccinated.
Methods
The study did not have a pre-registered protocol. The data were obtained from the Office for National Statistics of England, where they are freely available.15 The analyses were exploratory. To assess possible differences in non-COVID-19 and COVID-19 mortality rates, the age-adjusted mortality rates were extracted by age group (18 – 39 years, 40 – 49 years, 50 – 59 years, 60 – 69 years, 70 – 79 years, 80 – 89 years and 90 years or older) and by vaccination status (unvaccinated, vaccinated with one, two, three or four doses at least 21 days previously. The case numbers in the category “vaccinated within the last 21 days” were also available, but lower and therefore prone to outliers, so that the data analysis was restricted to those with a dose of vaccine given at least 21 days ago.
The age-adjusted non-COVID-19 mortality rate among the unvaccinated was set as the benchmark, assuming that COVID-19 vaccination should have no positive or negative effect on the age-adjusted non-COVID-19 mortality rate, resulting in similar rates in each age group regardless of the COVID-19 vaccination status.
Results
Benchmark rates of the COVID-19 unvaccinated
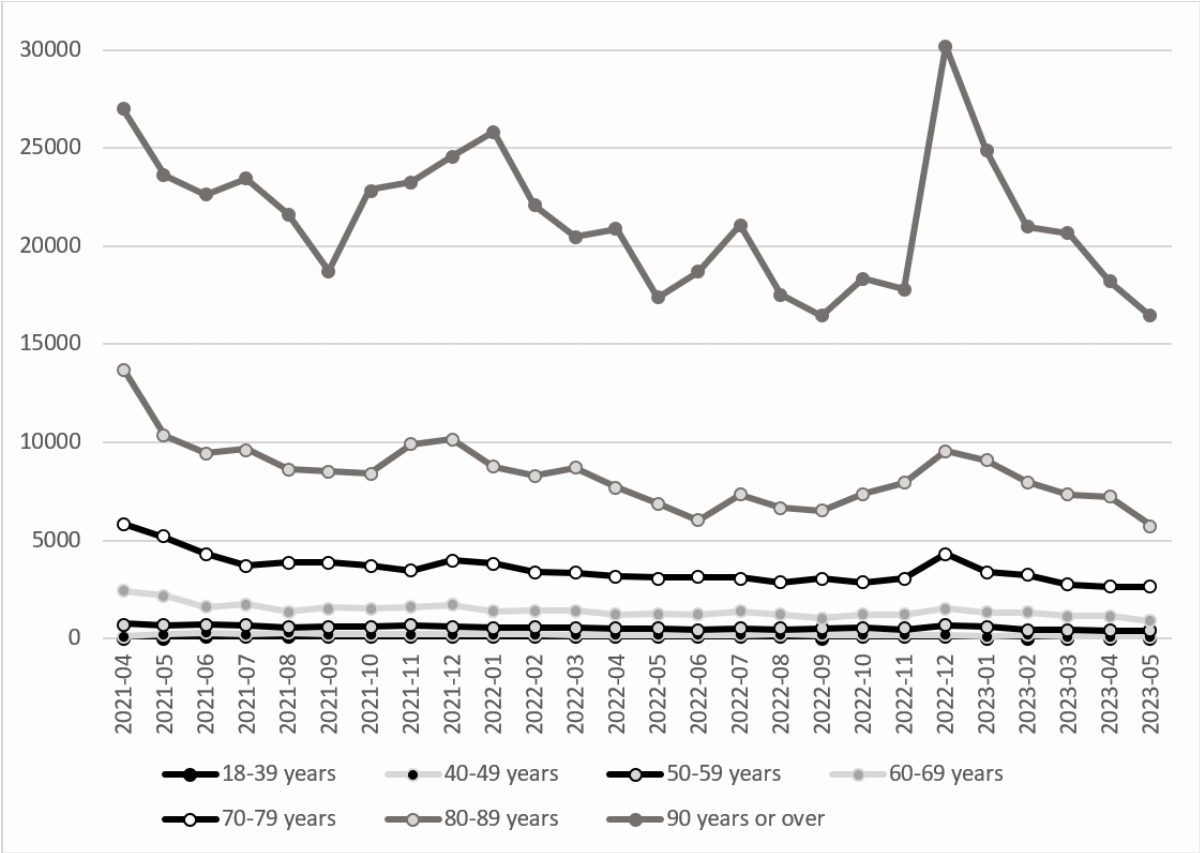
The age-standardized non-COVID-19 mortality rate per 100,000 was within a stable range in all age groups except the cohort aged 90 years and older, that showed peaks in mortality in mid-winter 2021 and 2022 (Figure 1). It was between 22.9 and 70.5 in the age group 18 – 39 years, between 100.9 and 278.5 in the age group 40 - 49 years, between 369.2 and 740.6 in the age group 50 - 59 years, between 894.6 and 2,425.2. in the age group 60 - 69 years, between 2,646.4 and 5,862.0 in the age group 70 - 79 years, between 5,767.2 and 13,745.6 in the age group 80 - 89 years and between 16,441.3 and 30,234.8 among those in the age group 90 years or older. A higher non-COVID-19 mortality rate per 100,000 was found for those aged 60 years or over during the winter period, indicating a seasonality in the non-COVID-19 mortality rate.
All age groups
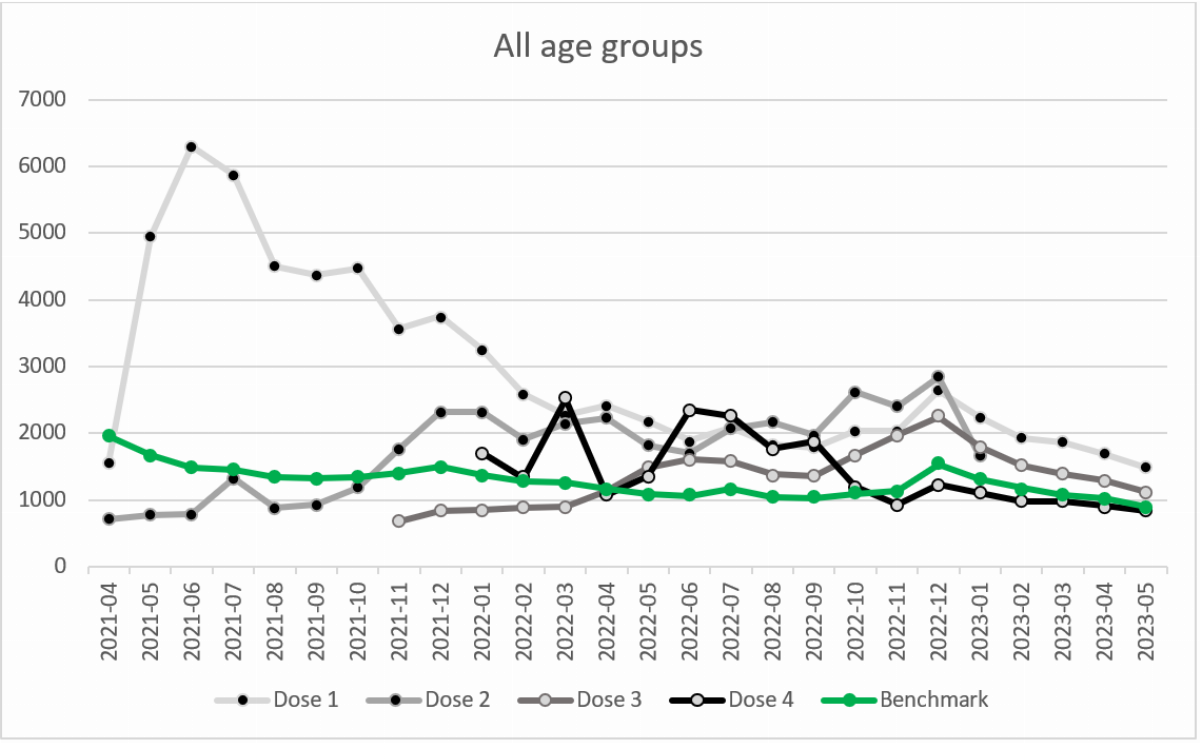
The age-standardized non-COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated ranged from 901.6 in May 2023 to 1956.3 in April 2021 (Figure 2). It was higher, ranging from +580.9 to +4809.4, compared with the unvaccinated in 25 of the 26 months among those who have received one dose of the vaccine. It was lower between April and October 2021 ranging from -123.4 to -1249.7, and higher between November 2021 and January 2023, ranging from +340.7 to +1522.2 among those who had received two doses of the vaccine. It was also lower between November 2021 and April 2022, ranging from -33.5 to -721.6, and higher between May 2022 and May 2023, ranging from +213.1 to +842.1 for those who had received three doses of the vaccine. And it was substantially higher in March 2022 (+1254.5) and between June and September 2022 (range between +714.1 and +1291.8) for those who had received four doses of the vaccine.
The age-standardized COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated ranged from 46.1 in May 2023 to 649.0 in January 2022. It was mostly lower (range between 1.6 and 575.4) among all those ever vaccinated (Figure S1).
Age group 18 – 39 years
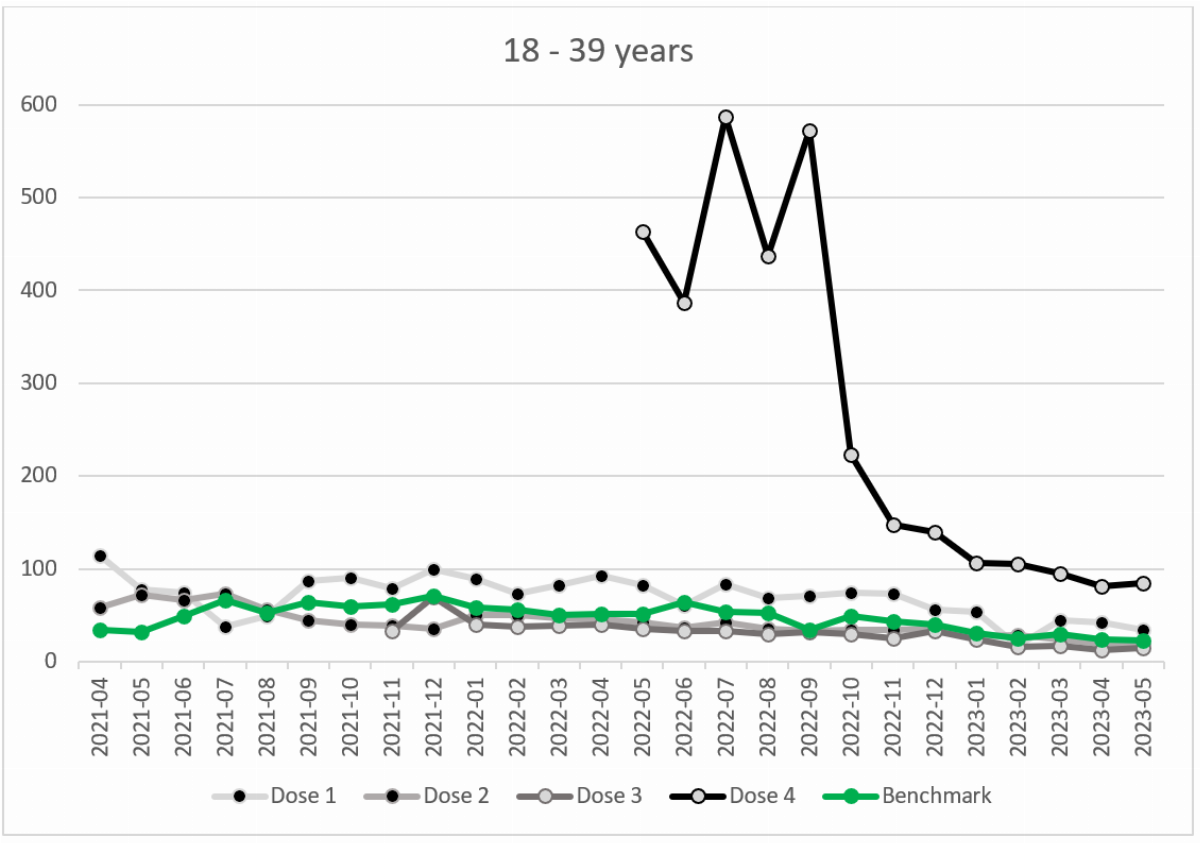
In the age group 18 – 39 years, the age-standardized non-COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated ranged from 22.9 in May 2023 to 70.5 in December 2021 (Figure 3). It was higher, ranging from +11.0 to +80.0, compared with the unvaccinated in 22 of the 26 months among those who have received one dose of the vaccine. It was higher between April and August 2021, ranging from +3.5 to +39.7, and lower between September 2021 and May 2023, ranging from -0.8 to -35.1, among those who had received two doses of the vaccine. It was also lower in all 19 months for those who had received three doses of the vaccine, ranging from -1.0 to -28.5. And it was substantially higher in all 13 months for those who had received four doses of the vaccine (range between +57.2 and +537.6).
The age-standardized COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated ranged from 0.6 in May 2021 to 27.6 in December 2021. It was consistently lower (range between 0.5 and 8.8) among all those ever vaccinated (Figure S2).
Age group 40 – 49 years
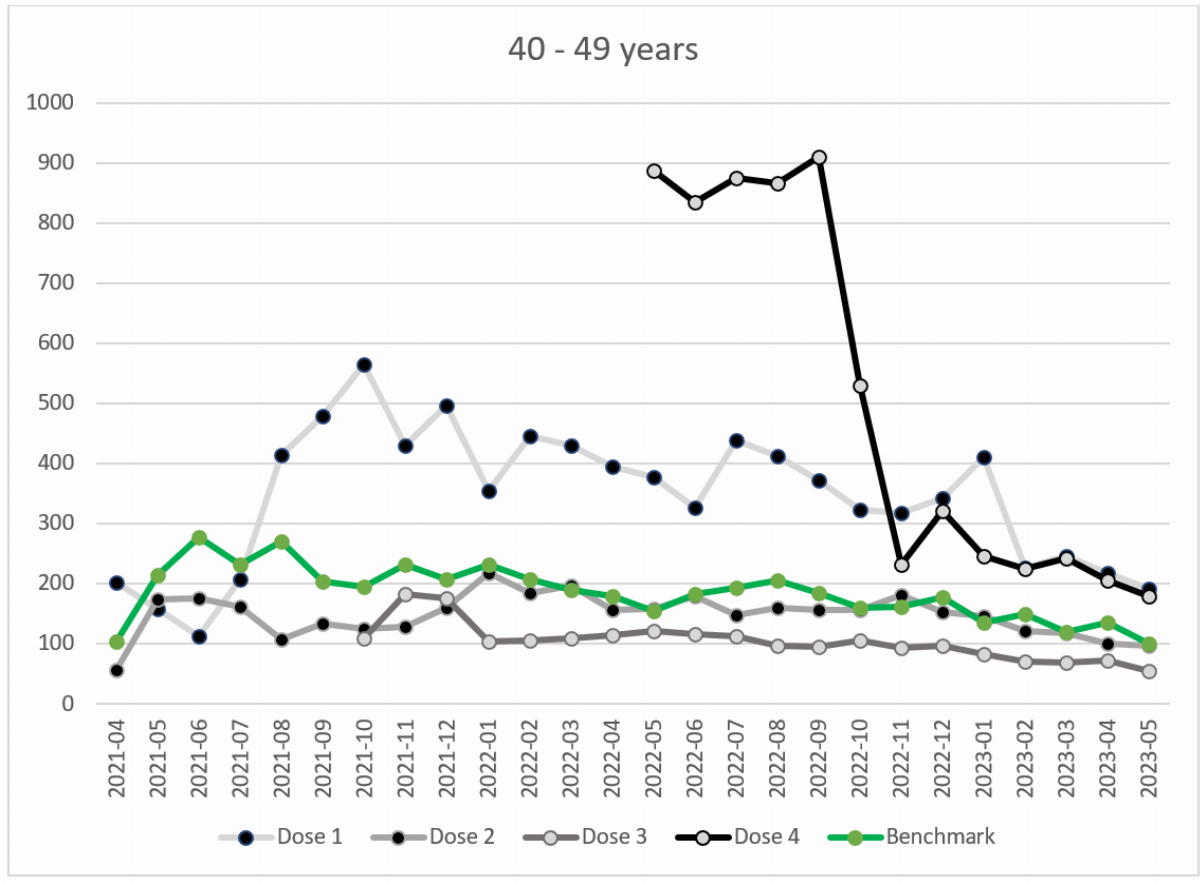
In the age group 40 – 49 years, the age-standardized non-COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated ranged from 100.9 in May 2023 to 278.5 in June 2021 (Figure 4). It was higher (range between +76.5 and +369.9) compared to the unvaccinated, in 23 of the 26 months among those who have received one dose of the vaccine. It was higher (range between +2.2 and +19.4) in four months and lower (range between -2.4 and -162.6) in 22 months among those who had received two doses of the vaccine. It was also lower (range between -30.3 and -127.8) at all 19 months for those who had received three doses of the vaccine. And it was substantially higher (range between +68.9 and +732.4) in all 13 months for those who had received four doses of the vaccine.
The age-standardized COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated showed seasonality, ranging from 5.1 in April 2021 to 134.1 in December 2021. With the dominance of the omicron variant in January 2022, age-standardized COVID-19 mortality rate was low ranging from 5.0 to 57.0. It was mostly lower among all those ever vaccinated until December 2021 (range between 2.8 and 37.9) but was in a similar range to the unvaccinated starting with the dominance of the omicron in January 2022 (Figure S3).
Age group 50 – 59 years
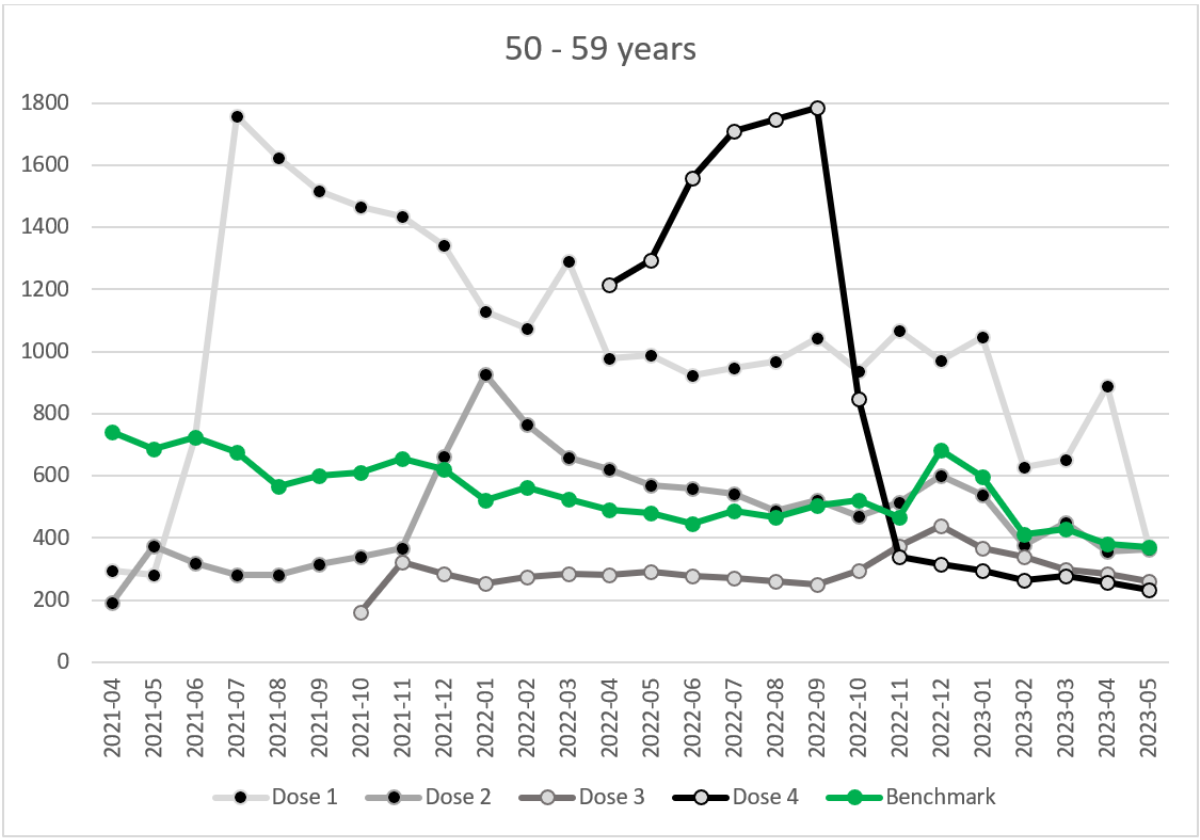
In the 50 – 59 age group, the age-standardized non-COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated ranged from 369.2 in May 2023 to 740.6 in April 2021 (Figure 5). It was higher (range between +4.8 and +1,080.7) compared with the unvaccinated in 23 of the 26 months among those who have received one dose of the vaccine. It was lower (range between -272.8 and -549.7) between April and November 2021, higher (range between +41.7 and +404.0) in the following eight months, and close to the benchmark in the last ten months among those who had received two doses of the vaccine. It was also lower in all 19 months for those who had received three vaccine doses (range between -72.7 and -450.6). And it was substantially higher (range between +324.2 and +1,280.5) between April and October 2022 and lower (range between -126.4 and -366.9) between November 2022 and May 2023 among those who had received four doses of the vaccine.
The age-standardized COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated was higher until March 2022, ranging from 28.7 in May 2021 to 327.9 in August 2021. After the dominance of the omicron variant, age-standardized COVID-19 mortality rate was lower, ranging mostly between 11.2 and 27.0. It was mostly lower among all those ever vaccinated until March 2022 (range between 2.5 and 214.0), but after the dominance of the omicron variant, it was in a similar range to the unvaccinated (Figure S4).
Age group 60 – 69 years
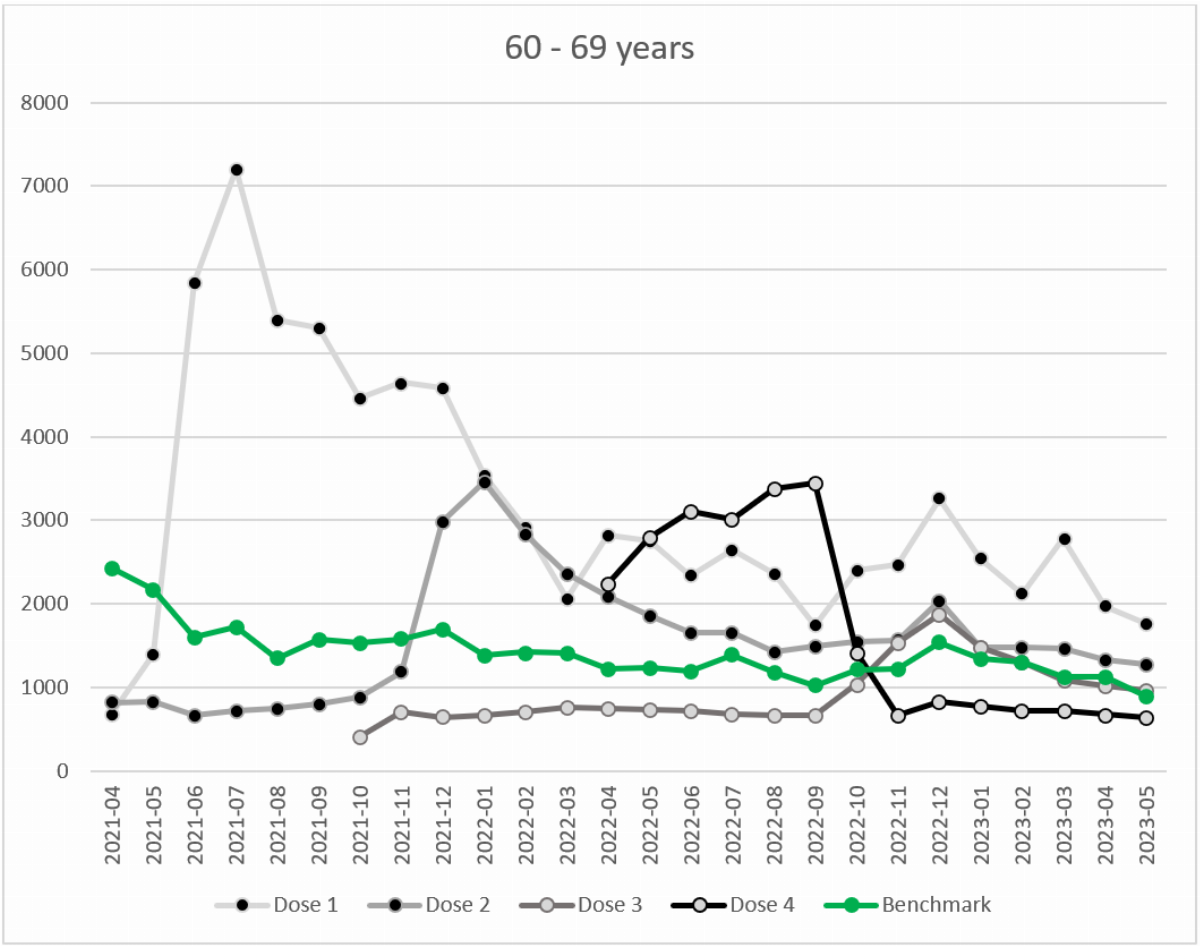
In the age group 60 – 69 years, the age-standardized non-COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated ranged from 894.6 in May 2023 to 2,425.2 in April 2021 (Figure 6). It was higher (range between +653.1 and +5,481.4) with a peak in the summer 2021 compared to the unvaccinated in 24 of the 26 months among those who have received one dose of the vaccine. It was lower (range between -391.6 and -1,608.0) between April and November 2021 and higher (range between +139.7 and +2,069.0) in the following 18 months among those who had received two doses of the vaccine. It was lower (range between -170.5 and -1,120.6) between October 2021 and October 2022 and close to the benchmark in the following seven months for those who had received three doses of the vaccine. And it was higher (range between +196.6 and +2,416.2) between April and October 2022 and lower (range between -259.5 and -716.0) between November 2022 and May 2023 for those who had received four doses of the vaccine.
The age-standardized COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated was higher until January 2022, ranging from 100.2 in May 2021 to 787.7 in December 2021. After the dominance of the omicron variant, age-standardized COVID-19 mortality rate was lower, ranging mostly between 42.7 and 145.7. It was mostly lower among all those ever vaccinated until January 2022, but after the dominance of the omicron variant, it was in a similar range to the unvaccinated, except for lower rates between February and September 2022 (dose 3) and for higher rates between April 2022 and May 2023 (dose 1) (Figure S5).
Age group 70 – 79 years
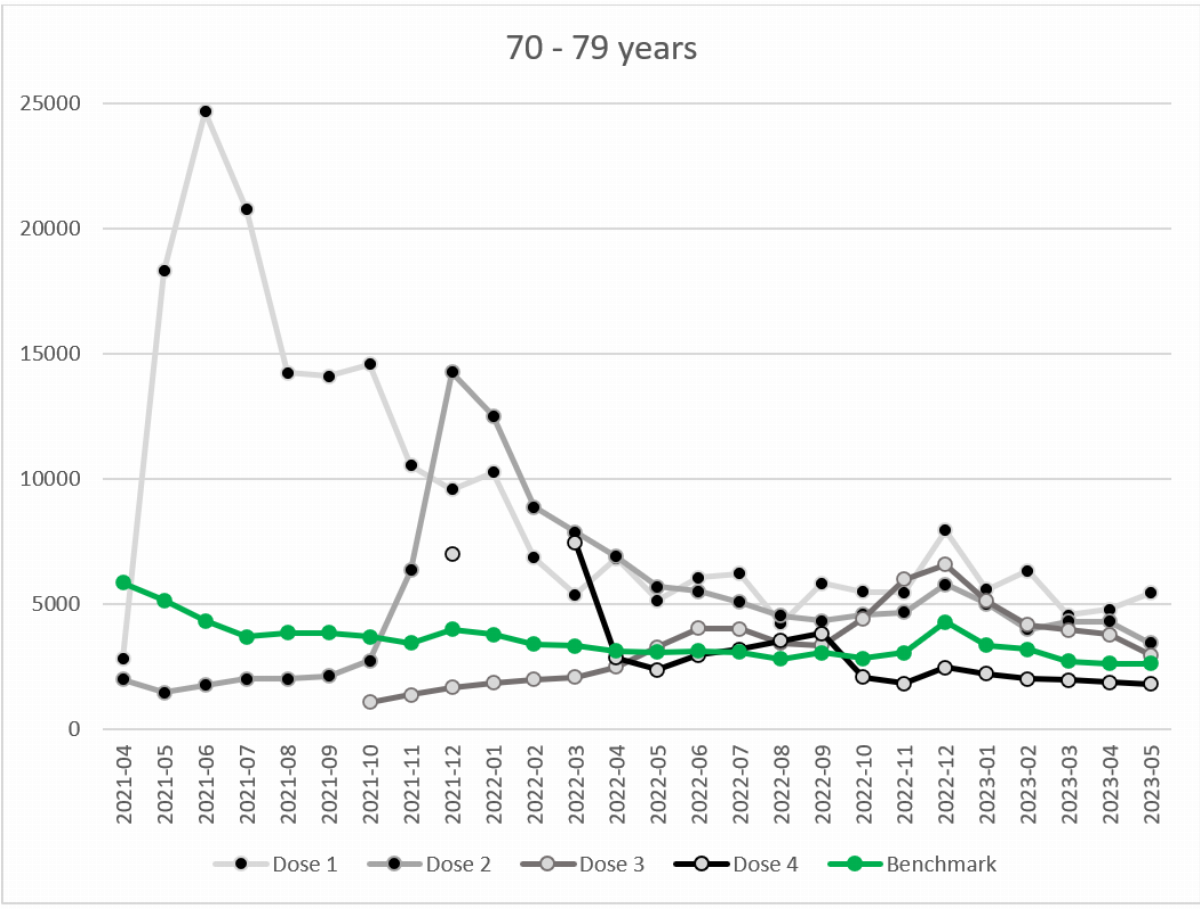
In the age group 70 – 79 years, the age-standardized non-COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated ranged from 2,646.4 in May 2023 to 5,862.0 in April 2021 (Figure 7). It was higher (range between +1,396.4 and +20,329.3) compared to the unvaccinated in 25 of the 26 months, with a peak in the summer 2021 among those who have received one dose of the vaccine. It was lower (range between -965.0 and -3,864.3) between April and October 2021 and higher (range between +788.5 and +10,250.9) in the following 19 months among those who had received two doses of the vaccine. It was lower between October 2021 and October 2022 (range between -965.0 and -3,864.4) with a peak in December 2021 and close to the benchmark in the last seven months for those who had received three doses of the vaccine. It was substantially higher (+4,134.2) in March 2022, close to the benchmark between April and October 2022 and lower (range between -746.4 and -1,818.4) between November 2022 and May 2023 for those who had received four doses of the vaccine.
The age-standardized COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated was higher until April 2022, ranging from 114.1 in May 2021 to 1,972.8 in January 2022. After the dominance of the omicron variant, age-standardized COVID-19 mortality rate was lower, ranging mostly between 108.9 and 444.7. For all those ever vaccinated it was mostly in a similar range to the unvaccinated, except for lower rates between April and December 2021 (dose 2) and for lower rates between October 2021 and May 2022 (dose 3) (Figure S6).
Age group 80 – 89 years
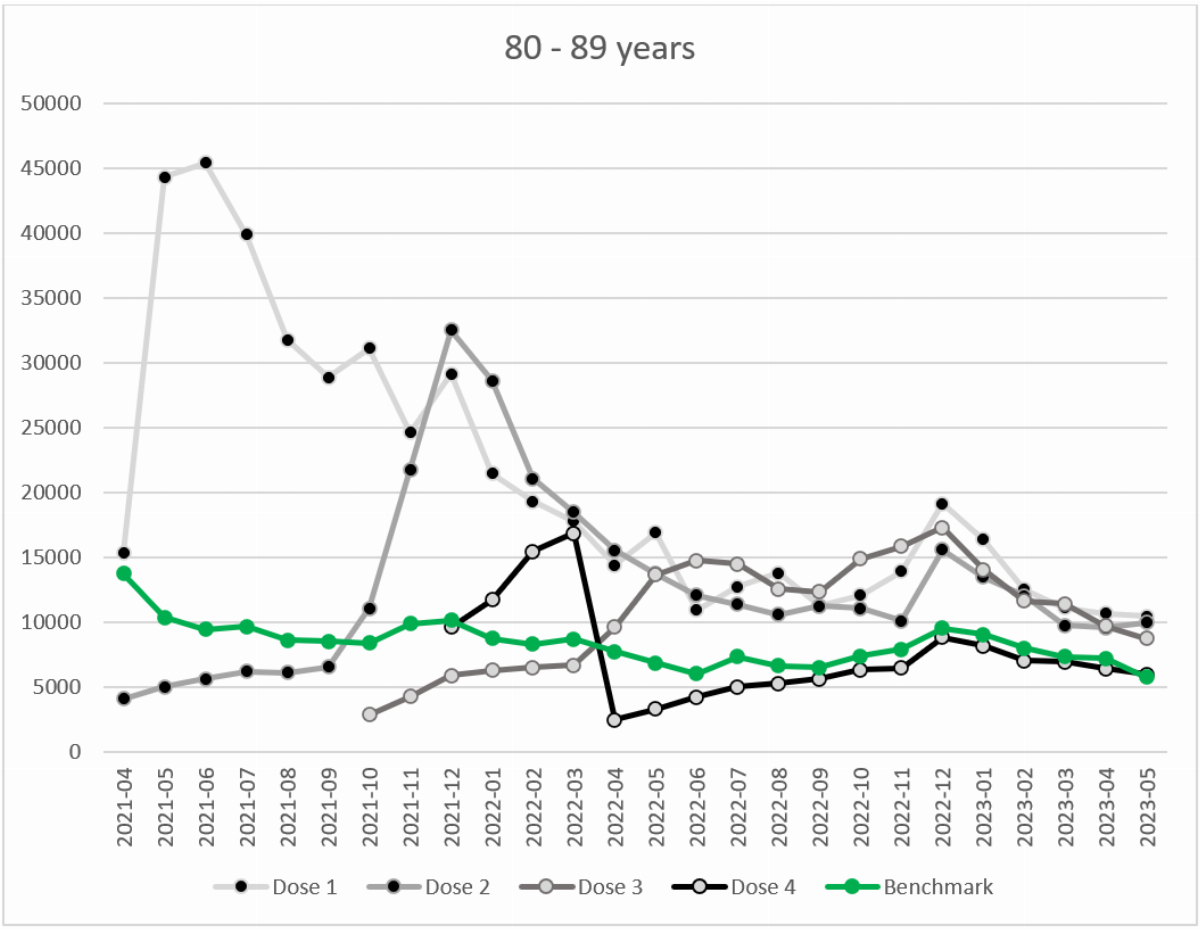
In the age group 80 – 89 years, the age-standardized non-COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated ranged from 5,767.2 in May 2023 to 13,745.6 in April 2021 (Figure 8). It was higher (range: +1,562.6 – +35,931.3) with a peak in the early summer 2021 compared to the unvaccinated in all of the 26 months among those who have received one dose of vaccine. It was lower (range: -1,969.7 – -9,636.7) between April and October 2021 and higher (range: +2,358.8 – +22,336.8) between November 2021 and May 2023 for those who had received two doses of the vaccine. It was lower (range: -1,791.0 – -5,581.5) between October 2021 and March 2022 and higher (range: +1,920.1 – +8,722.8) between April 2022 and May 2023 for those who had received three vaccine doses. It was higher between January and March 2022 (range: +2,961.2 – +8,130.7), lower in April (-5,239.2) and then approached the benchmark level for those who had received four doses of the vaccine.
The age-standardized COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated was higher between August 2021 and April 2022, ranging from 1781.6 in March 2022 to 4,131.3 in January 2022. After the dominance of the omicron variant, age-standardized COVID-19 mortality rate was lower, ranging mostly between 268.2 and 1,300.3. For all those ever vaccinated it was mostly in a similar range to the unvaccinated, except for lower rates between April and October 2021 (dose 2), lower rates between October 2021 and April 2022 (dose 3), and higher rates in January 2022 (doses 1 and 2) (Figure S7). Overall, COVID-19 vaccination was much less associated with the age-standardized COVID-19 mortality rate per 100,000 than with the non-COVID-19 mortality rate per 100,000.
Age group 90 years or over
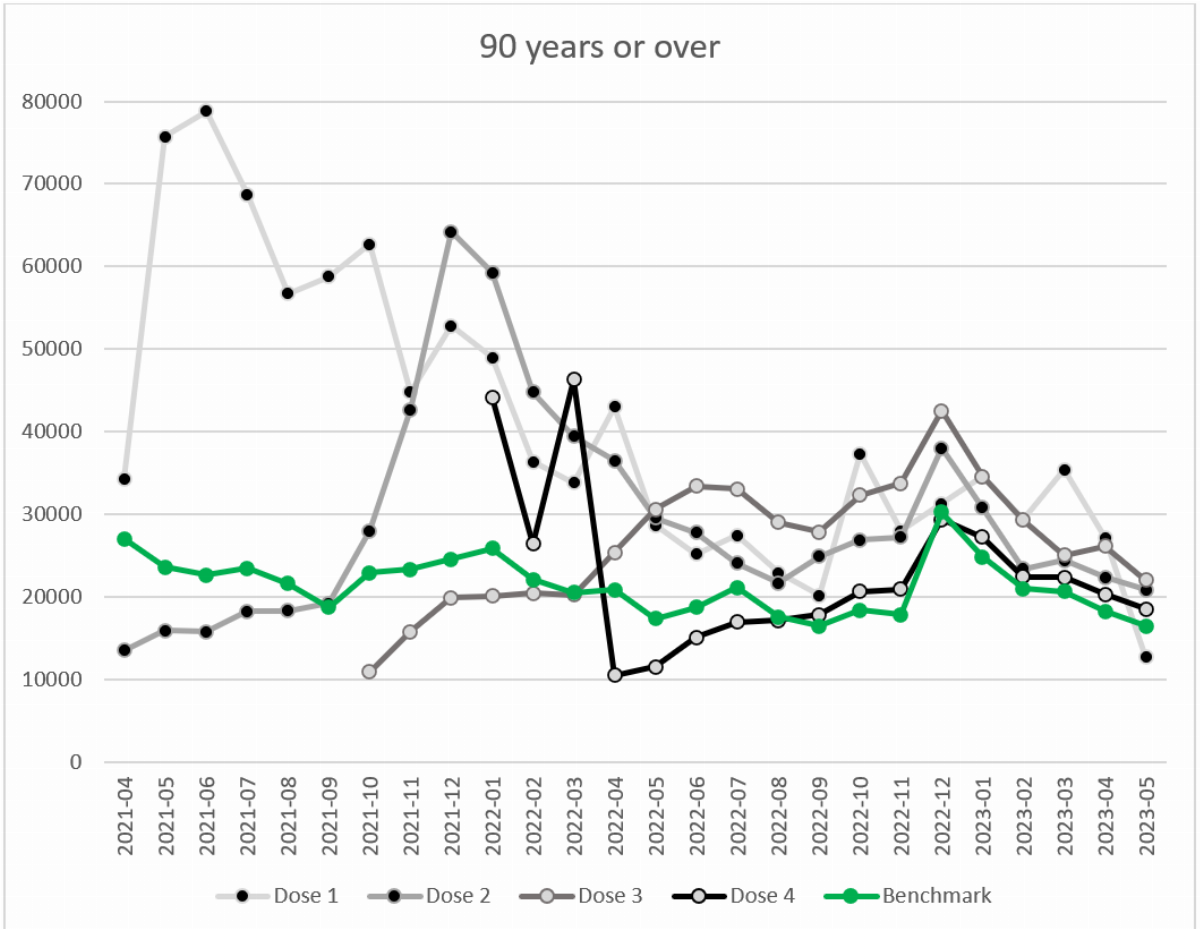
In the age group of 90 years and older, the age-standardized non-COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated ranged from 16,441.3 in May 2023 to 30,234.8 in December 2022 (Figure 9). It was higher (range: +1,009.8 – +56,184.6) compared to the unvaccinated in 25 of the 26 months among those who have received one dose of the vaccine. It was lower (range: -3,347.7 – -13,535.1) between April and August 2021 and higher (range: +458.8 – +39,592.1) between September 2021 and May 2023 for those who had received two vaccine doses. It was lower (range: -285.5 – -11,949.3) between April and September 2021 and higher (range: +4,494.4 – +15,971.1) between October 2021 and May 2023 for those who had received three vaccine doses. It was substantially higher in January 2022 (+18,350.2) and March 2022 (+25,825.2), lower in April 2022 (-10,360.4) and then approached the benchmark level for those who had received four vaccine doses.
The age-standardized COVID-19 mortality rate per 100,000 of the COVID-19 unvaccinated was higher between August 2021 and April 2022, ranging from 2,977.4 in September 2021 to 10,560.8 in January 2022. After the dominance of the omicron variant, age-standardized COVID-19 mortality rate was lower, ranging mostly between 788.3 and 3,313.3. For all those ever vaccinated it was mostly in a similar range to the unvaccinated, except for lower rates between April and December 2021 (dose 2), lower rates between October 2021 and April 2022 (dose 3), and a higher rate in January 2022 (dose 2) (Figure S8). Overall, COVID-19 vaccination was much less associated with the age-standardized COVID-19 mortality rate per 100,000 than with the non-COVID-19 mortality rate per 100,000.
Discussion
To our knowledge, this is the first report of non-COVID-19 age-adjusted mortality rates according to COVID-19 vaccination status. The rates were expected to be in a similar range in each age group, assuming that there is no association between the vaccination status and the non-COVID-19 mortality rates. However, this is not consistently the case. Several striking patterns emerged.
First, the age-adjusted non-COVID-19 mortality rates among those who have received 1 dose of the vaccine were mostly higher in all age groups. The most striking difference was found in those aged 70 – 79 years (maximum: 5.7-fold higher), followed by those aged 80 – 89 years (maximum: 4.8-fold higher) and those aged 60 – 69 years (maximum: 4.2-fold higher). The highest peaks were typically found in the first three months between April and July 2021. A further observation is that the peaks of elevated age-adjusted non-COVID-19 mortality rates appear to follow the vaccination rollout described by the National Audit Office in February 2022,16 with peaks in May 2021 among those aged 80 years or older, a peak in June May 2021 among those aged 70 - 79 year, and a delayed peak in July 2021 among those aged 50 – 69 years, providing further support for the COVID-19 vaccination as a possible cause of the elevated age-adjusted non-COVID-19 mortality rates (Figure S9).
Another pattern is that the age-adjusted non-COVID-19 mortality rates after dose 2 show peaks in those aged 70 – 79 years (maximum: 3.6-fold higher; December 2021), those aged 80 – 89 years (maximum: 3.3-fold higher; January 2022), those aged 90 years or older (maximum: 2.6-fold higher; December 2021), and those aged 60 – 69 years (maximum: 2.5-fold higher; January 2022). These results are supported by findings from Norway, where the vaccination campaign began in nursing home residents with the first vaccine-related death reported already on 4 January 2021. The number increased to 142 deaths by May 2021. Autopsies were performed in May 2021 on 100 deceased nursing home residents who died after receiving the COVID-19 vaccine, mostly 8 days after the injection. The average age was 87.7 years. In ten cases, the vaccination was probably the cause of death, and in 26 cases it was possibly the cause. The researchers concluded that in some cases, the vaccination may have accelerated the process of death that had already begun. They therefore recommended that the benefits and risks should be weighed carefully in each individual case, even in elderly and frail people.17 In Germany, deaths after vaccination of residents were reported from several nursing homes in the winter of 2021, but were not officially considered as potential serious adverse reactions. The population groups with the highest non-COVID-19 mortality rates without vaccination, with highly elevated non-COVID-19 mortality rates after dose 1, now also have a higher non-COVID-19 mortality rate after dose 2. Therefore, the higher non-COVID-19 mortality may possibly explain a relevant proportion of the excess deaths during this period.
The results are not easy to explain. The first two patterns may be explained by the assumption that those who preferred to not be vaccinated may have been very healthy, so that they thought they did not need the vaccine, resulting in a healthy non-vaccinee bias, especially in the elderly. In the absence of co-variate data on comorbidities and other variables that compare non-vaccinated with different dose vaccinated people, it is not possible to determine if the differences can be explained by the vaccination status or the comorbidities in the vaccinated populations. The results may also be explained by an vaccine-induced increased susceptibility to other diseases than COVID-19, which has raised the demand already to study the non-specific effects of mRNA vaccines on the overall mortality in depth.18 However, it has been reported from Japan that after mass vaccination with the third dose of mRNA vaccines in 2022, significant excess mortality was observed for all cancers and some specific cancers, including prostate cancer, pancreatic cancer and breast cancer.19 This is unlikely to explain a higher rate shortly after a vaccination, but may partly explain the increased rates associated with dose 3 in people aged 80 years and over from May 2022.
In rats, the mRNA vaccines mRNA1273 (Moderna) and BNT162b2 (BioNTech/Pfizer) were found to induce specific dysfunctions of the heart. mRNA1273 caused induced both arrhythmic and completely irregular contractions, while BNT162b2 increased cardiomyocyte contraction at the cellular level. Both changes can significantly increase the risk of acute cardiac events and may therefore explain the excess mortality after vaccination20 and the increase in “sudden unexpected deaths”. This may also partly explain the generally higher non-COVID-19 mortality rate in all age groups. Vaccine-associated myocarditis has also been described to be potentially fatal,21 with most hospitalized cases of myocarditis occurring among male adolescents.22
A third striking pattern are the higher age-adjusted non-COVID-19 mortality rates among those aged 18 – 39 years (maximum: 16.7 times higher), which decreased with increasing age, as shown for those aged 40 – 49 years (maximum: 5.7 times higher), those aged 50 – 59 years (maximum: 3.7 times higher) and those aged 60 – 69 years (maximum: 3.4 times higher). An assumed “non-healthy vaccinee bias” is not evident to appear only after dose 3. We currently have no medical explanation for this surprising finding. Moderna’s bivalent booster vaccine was approved in the UK in August 2022, so that it may only explain the increased rates after August 2022, but not those between April and July 2022.
Age-standardized COVID-19 mortality rates were mostly only lower among the ever vaccinated before the dominance of the omicron variant. A lower vaccine efficacy against the omicron variant has been reported, which includes a lower effectiveness against death.23 The comparison between the age-standardized non-COVID-19 mortality rates per 100,000 and the age-standardized COVID-19 mortality rates per 100,000 shows that both the level of non-COVID-19 mortality and the vaccine-associated increase in non-COVID-19 mortality were higher compared to the COVID-19 mortality and the vaccine-associated decrease in COVID-19 mortality, suggesting an overall negative benefit-risk-evaluation for the COVID-19 vaccines regarding mortality.
However, our analyses have relevant limitations. First, we were unable to adjust for comorbidities, sex, socioeconomic and other risk factors that affect mortality risk in the general population. In addition, it is possible that vaccinated and unvaccinated individuals may have different age distributions (even more so in the upper age stratum), and thus this crude age adjustment does not fully adjust for age.
Second, there may also be an important selection bias, especially among the elderly. Some of those who died may have been so ill that they were unable or unwilling to receive a second dose if they were thought to be terminally ill, or if they were unable to tolerate the first dose because of their general weakness. People with two doses may have had, on average, more comorbidities than the unvaccinated. The older people who chose not to be vaccinated may have been mostly healthy. Although this is only speculation, it may provide an alternative explanation for the increased age-adjusted non-COVID-19 mortality among those who received the COVID-19 vaccine.
Third, selection biases such as the healthy vaccinee type or, conversely, healthy non-vaccinee type, may also have affected the results. This type of bias is different among countries, settings, time periods, and health systems. For example, countries like Israel, Austria and USA have documented mostly healthy vaccinee bias rather than healthy non-vaccinee bias.24,25,26 Possibly the results presented here may be explained by a healthy non-vaccinee bias.
Fourth, it is possible that COVID-19 and non-COVID-19 deaths were misclassified to an unknown extent. However, the possible effect of misclassification on the overall results cannot be predicted.
In 2022, an estimate of 18.2 million COVID-19 deaths worldwide was made for the years 2020 and 2021, despite a number of confirmed COVID-19-associated deaths of 5.9 million. It is important to note that the number of "confirmed" COVID-19-associated deaths is likely to be overestimated because of the April 2020 guidelines from the WHO.27 It states: “With reference to section 4.2.3 of volume 2 of ICD-10, the purpose of mortality classification (coding) is to produce the most useful cause of death statistics possible. Thus, whether a sequence is listed as ‘rejected’ or ‘accepted’ may reflect interests of importance for public health rather than what is acceptable from a purely medical point of view. Therefore, always apply these instructions, whether they can be considered medically correct or not.” This invites the non-medically correct attribution of a death to COVID-19 if it is judged to be "in the interest of public health". The April 2020 guidelines also state that “a manual plausibility check is recommended for certificates where COVID-19 is reported, in particular for certificates where COVID-19 was reported but not selected as the underlying cause of death for statistical tabulation.” In The Netherlands it has been argued that strict compliance to these WHO guidelines may have contributed to a overreporting of COVID-19 deaths.28
But regardless of the unanswered questions about confirmed COVID-19 deaths, the even higher estimate of 18.2 million COVID-19 deaths worldwide was based on total excess mortality, although there is no evidence to support the simplified approach of considering total excess mortality as COVID-19 mortality.29 Based on the results of this study, it seems reasonable to assume that an unknown proportion of the additional 12.3 million deaths may be explained by the COVID-19 vaccination starting in 2021, based on the substantially higher age-adjusted non-COVID-19 mortality rates after dose 1 between April and December 2021 among those aged 50 years and older. This assumption is further supported by the finding that the participants of the phase 3 randomized controlled trial of BNT162b2, when followed up for 6 months instead of 20 weeks as previously published after completing the vaccination,30 found 21 deaths among the vaccinated and 17 deaths among the unvaccinated.31 The authors found evidence of an over 3.7-fold increase in number of deaths due to cardiac events in the BNT162b2 vaccinated individuals compared to those who received only the placebo. In addition, a fatal case post vaccination has been reported who still had vaccine in the right ventricle including multiple healing myocardial injuries dating two to three weeks prior to death and overlapping with the time of application of the second vaccine injection 19 days prior to death.32
We acknowledge that the excess deaths are subject to many uncertainties and that causal explanations require great caution.33 However, despite the many uncertainties, it should be considered that the COVID-19 vaccines may have contributed to the excess mortality, to whatever extent.
Conclusions
Although a causal relationship between excess mortality and vaccination against COVID-19 has not been firmly established, a higher age-adjusted non-COVID-19 mortality rates among the COVID-19 vaccinated in several age groups was found that requires further research
References
Mostert S, Hoogland M, Huibers M, Kaspers G. Excess mortality across countries in the Western World since the COVID-19 pandemic: ‘Our World in Data’ estimates of January 2020 to December 2022. BMJ Public Heal [Internet]. 2024 May 3 [cited 2024 Jun 4];2(1):e000282. Available from: https://bmjpublichealth.bmj.com/content/2/1/e000282
Ioannidis JPA, Zonta F, Levitt M. Variability in excess deaths across countries with different vulnerability during 2020-2023. Proc Natl Acad Sci U S A [Internet]. 2023 [cited 2024 Jun 4];120(49):e2309557120. Available from: https://pubmed.ncbi.nlm.nih.gov/38019858/
Kuhbandner C, Reitzner M. Estimation of Excess Mortality in Germany During 2020-2022. Cureus. 2023;15(5):e39371.
Morfeld P, Timmermann B, Lewis P, Erren T. Increased Mortality in Germany and in the Individual German States During the SARS-CoV-2/COVID-19 Pandemic in 2020 and 2021. Dtsch Arztebl Int [Internet]. 2022 Aug 22 [cited 2024 Apr 17];119(33–34):560–1. Available from: https://pubmed.ncbi.nlm.nih.gov/36422870/
Kuhbandner C, Reitzner M. Differential Increases in Excess Mortality in the German Federal States During the COVID-19 Pandemic. Researchgate [Internet]. 2024 [cited 2024 Apr 17];preprint. Available from: https://www.researchgate.net/publication/378124684_Differential_Increases_in_Excess_Mortality_in_the_German_Federal_States_During_the_COVID-19_Pandemic
Lytras T, Athanasiadou M, Demetriou A, Stylianou D, Heraclides A, Kalakouta O. Lack of association between vaccination rates and excess mortality in Cyprus during the COVID-19 pandemic. Vaccine [Internet]. 2023 May 2 [cited 2024 Jun 3];41(18):2941–6. Available from: https://pubmed.ncbi.nlm.nih.gov/37012116/
Economidou EC, Markou N, Prokopi K, Avraam D, Soteriades ES. Excess Mortality in Cyprus during the COVID-19 Epidemic. J Community Med Public Heal. 2024;8(1):407.
Haklai Z, Goldberger NF, Gordon ES. Mortality during the first four waves of COVID-19 pandemic in Israel: March 2020-October 2021. Isr J Health Policy Res [Internet]. 2022 Dec 1 [cited 2024 Jun 5];11(1):24. Available from: https://pubmed.ncbi.nlm.nih.gov/35642003/
Alicandro G, Remuzzi G, Centanni S, Gerli A, La Vecchia C. Excess total mortality during the Covid-19 pandemic in Italy: updated estimates indicate persistent excess in recent months. Med Lav [Internet]. 2022 Apr 26 [cited 2024 Jun 5];113(2):e2022021. Available from: https://pubmed.ncbi.nlm.nih.gov/35481574/
Faust JS, Renton B, Chen AJ, Du C, Liang C, Li SX, et al. Uncoupling of all-cause excess mortality from COVID-19 cases in a highly vaccinated state. Lancet Infect Dis [Internet]. 2022 Oct 1 [cited 2024 Jun 5];22(10):1419–20. Available from: https://pubmed.ncbi.nlm.nih.gov/36007530/
Liu JY, Chen TJ, Hou MC. Does COVID-19 vaccination cause excess deaths? J Chin Med Assoc [Internet]. 2021 Sep 1 [cited 2024 Jun 3];84(9):811–2. Available from: https://pubmed.ncbi.nlm.nih.gov/34524211/
Wadman M. Scientists quit journal board, protesting ‘grossly irresponsible’ study claiming COVID-19 vaccines kill. Science (80- ). 2021 Jul 1;online.
Sessa F, Salerno M, Esposito M, Di Nunno N, Zamboni P, Pomara C. Autopsy Findings and Causality Relationship between Death and COVID-19 Vaccination: A Systematic Review. J Clin Med [Internet]. 2021 Dec 1 [cited 2022 Aug 9];10(24):5876. Available from: /pmc/articles/PMC8709364/
Häring N. Karl Lauterbach und die Übersterblichkeit [Internet]. 2023 [cited 2023 Jun 30]. Available from: https://norberthaering.de/news/lauterbach-uebersterblichkeit/
Office for National Statistics. Deaths by vaccination status, England [Internet]. 2023 [cited 2024 May 29]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/deathsbyvaccinationstatusengland
Davies G. The rollout of the COVID-19 vaccination programme in England [Internet]. 2022 [cited 2025 Feb 6]. Available from: https://www.nao.org.uk/wp-content/uploads/2022/02/The-rollout-of-the-COVID-19-vaccination-programme-in-England.pdf
Wyller TB, Kittang BR, Ranhoff AH, Harg P, Myrstad M. Nursing home deaths after COVID-19 vaccination. Tidsskr Nor Laegeforen. 2021/05/22. 2021;141.
Rubio-Casillas A, Rodriguez-Quintero CM, Redwan EM, Gupta MN, Uversky VN, Raszek M. Do vaccines increase or decrease susceptibility to diseases other than those they protect against? Vaccine [Internet]. 2024 Jan 25 [cited 2024 May 29];42(3):426–40. Available from: https://pubmed.ncbi.nlm.nih.gov/38158298/
Gibo M, Kojima S, Fujisawa A, Kikuchi T, Fukushima M, GIBO M, et al. Increased Age-Adjusted Cancer Mortality After the Third mRNA-Lipid Nanoparticle Vaccine Dose During the COVID-19 Pandemic in Japan. Cureus [Internet]. 2024 Apr 8 [cited 2024 Apr 17];16(4):e57860. Available from: https://www.cureus.com/articles/196275-increased-age-adjusted-cancer-mortality-after-the-third-mrna-lipid-nanoparticle-vaccine-dose-during-the-covid-19-pandemic-in-japan
Schreckenberg R, Woitasky N, Itani N, Czech L, Ferdinandy P, Schulz R. Cardiac side effects of RNA-based SARS-CoV-2 vaccines: Hidden cardiotoxic effects of mRNA-1273 and BNT162b2 on ventricular myocyte function and structure. Br J Pharmacol [Internet]. 2024 Feb 1 [cited 2024 May 24];181(3):345–61. Available from: https://pubmed.ncbi.nlm.nih.gov/37828636/
Hulscher N, Hodkinson R, Makis W, McCullough PA. Autopsy findings in cases of fatal COVID-19 vaccine-induced myocarditis. ESC Hear Fail [Internet]. 2024 [cited 2024 Jun 3]; Available from: https://pubmed.ncbi.nlm.nih.gov/38221509/
Montag K, Kampf G. Hospitalised Myocarditis and Pericarditis Cases in Germany Indicate a Higher Post-Vaccination Risk for Young People Mainly after COVID-19 Vaccination. J Clin Med [Internet]. 2022 Oct 1 [cited 2024 Jun 3];11(20):6073. Available from: https://pubmed.ncbi.nlm.nih.gov/36294393/
Paul P, El-Naas A, Hamad O, Salameh MA, Mhaimeed N, Laswi I, et al. Effectiveness of the pre-Omicron COVID-19 vaccines against Omicron in reducing infection, hospitalization, severity, and mortality compared to Delta and other variants: A systematic review. Hum Vaccin Immunother [Internet]. 2023 [cited 2024 Jun 4];19(1):2167410. Available from: https://pubmed.ncbi.nlm.nih.gov/36915960/
Chalupka A, Riedmann U, Richter L, Chakeri A, El-Khatib Z, Sprenger M, et al. Effectiveness of the First and Second Severe Acute Respiratory Syndrome Coronavirus 2 Vaccine Dose: A Nationwide Cohort Study From Austria on Hybrid Versus Natural Immunity. Open Forum Infect Dis [Internet]. 2024;11(10):ofae547. Available from: https://doi.org/10.1093/ofid/ofae547
Høeg TB, Duriseti R, Prasad V. Potential “Healthy Vaccinee Bias” in a Study of BNT162b2 Vaccine against Covid-19. N Engl J Med. 2023;389(3):284–5.
Xu S, Huang R, Sy LS, Glenn SC, Ryan DS, Morrissette K. COVID-19 Vaccination and Non – COVID-19 Mortality Risk — Seven Integrated Health Care Organizations ,. MMWR - Morb Mortal Wkly Rep. 2021;70(43):1520–4.
WHO. INTERNATIONAL GUIDELINES FOR CERTIFICATION AND CLASSIFICATION (CODING) OF COVID-19 AS CAUSE OF DEATH Based on ICD International Statistical Classification of Diseases [Internet]. 2020 [cited 2023 Aug 3]. Available from: https://www.who.int/docs/default-source/classification/icd/covid-19/guidelines-cause-of-death-covid-19-20200420-en.pdf
Smulders M. Oversterfte: met of door covid-19? Med Contact (Bussum). 2024;79(5):18–21.
Wang H, Paulson KR, Pease SA, Watson S, Comfort H, Zheng P, et al. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020-21. Lancet (London, England) [Internet]. 2022 Apr 16 [cited 2024 May 29];399(10334):1513–36. Available from: https://pubmed.ncbi.nlm.nih.gov/35279232/
Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med. 2020/12/11. 2020;383(27):2603–15.
Michels C, Perrier D, Kunadhasan J, Clark E, Gehrett J, Gehrett B, et al. Forensic analysis of the 38 subject deaths in the 6-Month Interim Report of the Pfizer/BioNTech BNT162b2 mRNA Vaccine Clinical Trial. Int J Vaccine Theory, Pract Res. 2023;3(1):973–1008.
Krauson AJ, Casimero FVC, Siddiquee Z, Stone JR. Duration of SARS-CoV-2 mRNA vaccine persistence and factors associated with cardiac involvement in recently vaccinated patients. NPJ vaccines [Internet]. 2023 Dec 1 [cited 2024 Jun 19];8(1):141. Available from: https://pubmed.ncbi.nlm.nih.gov/37758751/
Ioannidis JPA, Zonta F, Levitt M. Flaws and uncertainties in pandemic global excess death calculations. Eur J Clin Invest. 2023;53(8):e14008.
