Abstract
Editor's Note: The following research article is an accepted manuscript awaiting peer review. Reviews of this article are forthcoming.
Background: COVID-19 vaccines have been administered to children worldwide. Investigating potential rare adverse events to the vaccine require post-marketing surveillance. Health registries can be useful tools.
Objective: We aimed to assess the potential for identifying self-reported rare adverse events in health registries.
Methods: A case-series was established via telephone interviews with parents of 21 Danish children aged 5-17, who had experienced new onset symptoms following Pfizer BNT162b2 vaccination, perceived by parents to be attributable to the vaccination. Participants were recruited via social media.
Results: All children had been vaccinated with Pfizer BNT162b2; 11 (52%) experienced new onset symptoms after dose 1 and 10 (47%) after dose 2. Nine (43%) had diagnoses that shared features of autoimmune illnesses; six (29%) had long-lasting infectious symptoms; 17 (81%) had an identifiable ICD-10 code.
Discussion and conclusion: The self-reported adverse events varied largely in their presentation; however, most were autoimmune or infectious. The present study does not establish any causal relations between COVID-19 vaccines and the observed diseases. The experienced diseases and symptoms can be difficult to identify in health registers, due to variation in their timing and diagnostic coding. It could be relevant to group rare diseases when conducting register studies.
Keywords: COVID-19, mRNA vaccine, autoimmunity, children, adverse events, non-specific effects.
1. Introduction
More than half of the world’s population has been immunized with at least one dose of SARS-CoV-2 (COVID-19) vaccine.1 The most common administered vaccine types in European children and adolescents are messenger RNA (mRNA) vaccines, including Pfizer (Comirnaty, BNT162B2) and Moderna (Spikevax, mRNA-1273).2 In Denmark, up to 80% of children aged 5-17 years received at least one dose and the vast majority were vaccinated with the Pfizer vaccine; only ~1000 children received Moderna.
The phase 3 mRNA trials enrolled a total of approximately 25,000 children aged 6 months to 17 years.3 Few serious adverse events (SAEs) were observed.4,5,6,7,8,9 Post-marketing follow-up detected an increased risk of post-vaccination myocarditis at a rate of about 1/3000 in adolescent males after the second dose of Pfizer.10
Rare adverse events can be particularly difficult to discover in phase 3 trials due to a limitation on study population sizes and duration of follow-up and may require post-marketing studies.11,12 Such studies could be based on national health registers in countries like Denmark, with an extensive public funded health care system and well-documented registers, linking information on health care utilization, socio-economy, general demographics, etc., on an individual level via a personal identification number.13,14,15,16
In the present paper, we aimed to evaluate the challenges in identifying rare adverse events using health registry data.
We established a case-series by conducting interviews with parents of children experiencing new-onset disease following immunization with an mRNA COVID-19 vaccine and performed a descriptive analysis of the reported conditions, where we consider the timing and nature of these conditions including disease category based on the provided ICD-10 codes (if any).
We did not aim for representativeness of possible adverse events following vaccination but assessed a sample of experienced adverse events in children believed by their parents to be related to the mRNA COVID-19 vaccines. Also, we did not aim to establish causal links between COVID-19 vaccines and the reported adverse events as doing so based on individual cases is not possible.
2. Methods
The study was conducted in Denmark, where COVID-19 vaccines to children were introduced in May 2021 for the 16-19-year-olds, July 2021 for the 12–15-year-olds, and in November 2021 for the 5–11-year-olds. From July 2022, COVID-19 vaccines have not been offered to children under 18 years of age Denmark without a physician’s prescription.
The aim of the study did not require a representative sample of those with self-reported adverse events. Participants were recruited through social media posts on Facebook, LinkedIn, and Twitter. Inclusion criteria were as follows: 1) The child had received the implicated vaccination prior to turning 18 years of age, 2) The child had experienced onset of new symptoms following receipt of a COVID-19 vaccine, and 3) The parent/guardian attributed the new symptom(s) to the vaccination.
Telephone interviews were conducted between March and June 2023. The list of questions is shown in the Supplementary Material. Questions included time of vaccination, time of positive COVID-tests (if such had been performed), the symptoms experienced by the child after receiving COVID-19 vaccine, how long post-vaccination and how long post-positive COVID-19 test (if applicable) these symptoms occurred. Specifically, regarding contact with the healthcare system, parents were asked about healthcare/hospital visits, ICD-10 diagnosis assigned at hospital encounters (if any) and whether they had reported the symptoms/disease to the Danish Medicines Agency and/or the Danish Patient Compensation.
In Denmark, all patients examined in a hospital setting are registered in the Danish National Health Registers, including the ICD-10 diagnoses related to the contact on an individual level.15 Diagnoses from General practitioners (GPs) and private practicing medical specialists are currently not available for research from the national registers. For the present study, data on medical history was provided by the parents, and not obtained via the national registers.
In addition to the interviews, we conducted a post-hoc literature search, including post-marketing surveillance studies and reports, reviews and case reports to investigate if any of the reported diseases had been described as possibly associated with the vaccines, and what the level of evidence for this was. This search was done using PubMed and included studies in English published from January 2020 to March 2025.
3. Ethics
The study was approved by the Regional Legal Services (SDU RIO, notification number 11.883) and the Research Ethics Committee (SDU REC, approval ID 23/19402). Written informed consent was obtained from the participants to publish this paper.
4. Results
A total of 25 people contacted us for study participation, and 21 children and adolescents were included. Two children were excluded (one with mild fever on the day of vaccination as only symptom, and one who was not vaccinated but had symptoms of Long-COVID), and two adults with post-vaccination symptoms were excluded due to the age restrictions.
Table 1 presents characteristics: 14 (67%) were female, the median age at first COVID-19 vaccine was 13 years (range 6 to 17 years). All children had received the Pfizer vaccine. Seven (33%) had documented prior or simultaneous positive PCR test for COVID-19 by the time of either COVID-19 vaccination. The table also outlines visits to GPs, private practicing medical specialists, and hospital departments related to the experienced symptoms along with previous vaccination history and baseline health information.
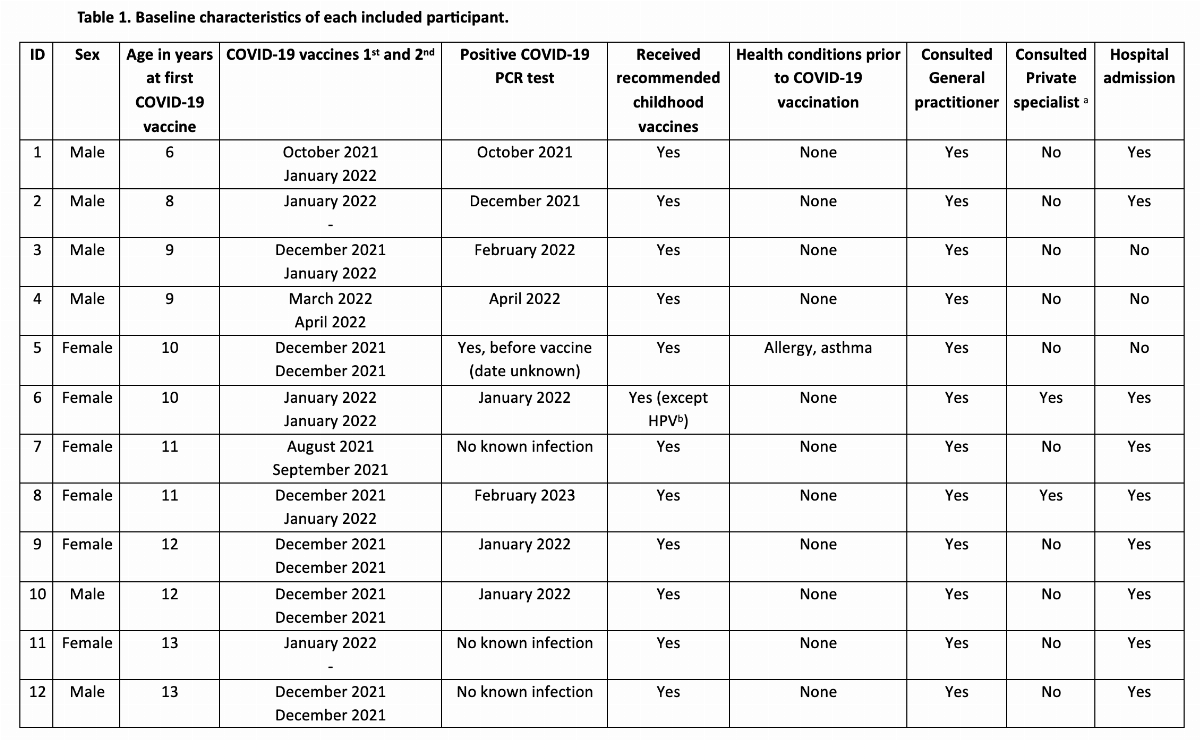
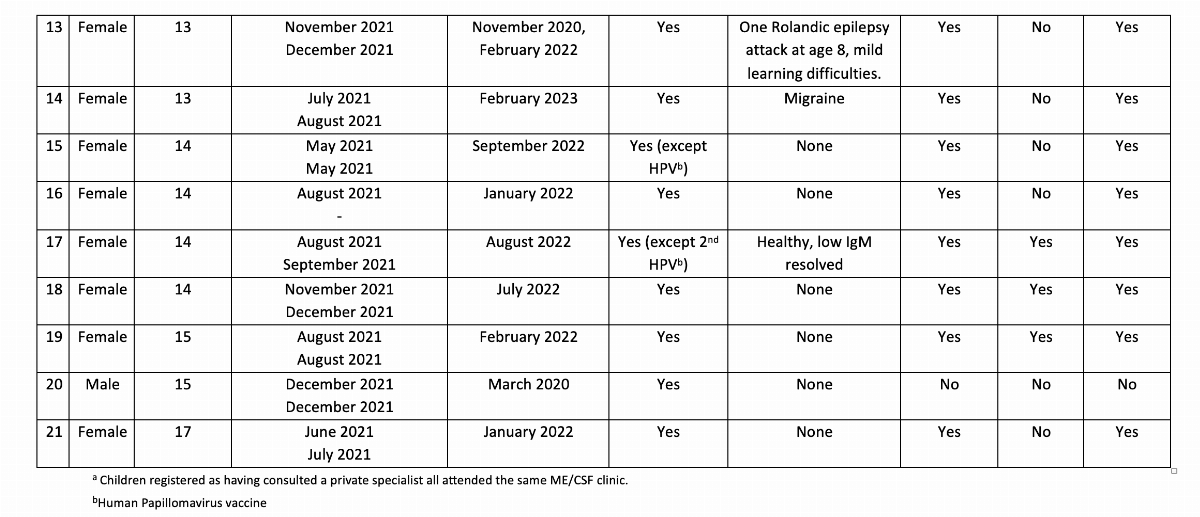 Prior to being vaccinated with an mRNA COVID-19 vaccine, all children had received all recommended childhood vaccines according to the Danish Childhood Vaccination Program,17 with the exception of three children not receiving all the vaccines against human papillomavirus (HPV) recommended at age 12. No adverse events from any of the previously administered vaccines were reported by parents. 17 children (81%) had no known underlying health conditions prior to being vaccinated. Participant 5 had pre-existing asthma and allergy, participant 13 had one previous Rolandic epilepsy attack, participant 14 had migraines, and participant 17 had prior history of low immunoglobulin M level, now resolved.
Prior to being vaccinated with an mRNA COVID-19 vaccine, all children had received all recommended childhood vaccines according to the Danish Childhood Vaccination Program,17 with the exception of three children not receiving all the vaccines against human papillomavirus (HPV) recommended at age 12. No adverse events from any of the previously administered vaccines were reported by parents. 17 children (81%) had no known underlying health conditions prior to being vaccinated. Participant 5 had pre-existing asthma and allergy, participant 13 had one previous Rolandic epilepsy attack, participant 14 had migraines, and participant 17 had prior history of low immunoglobulin M level, now resolved.
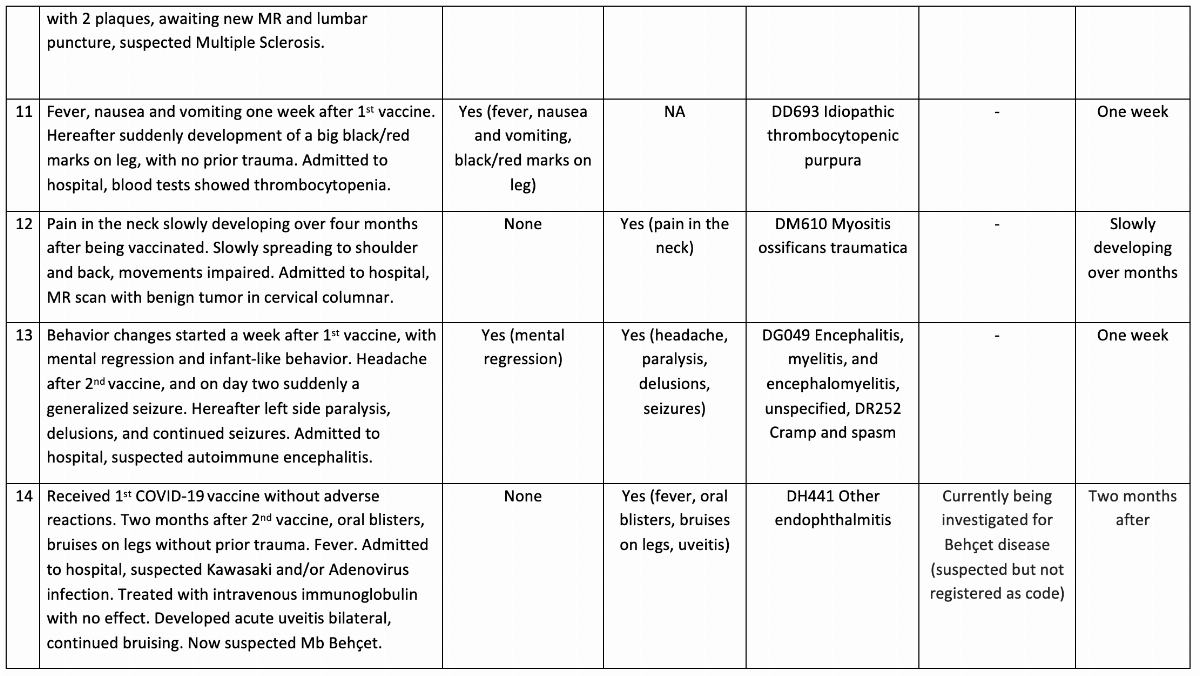
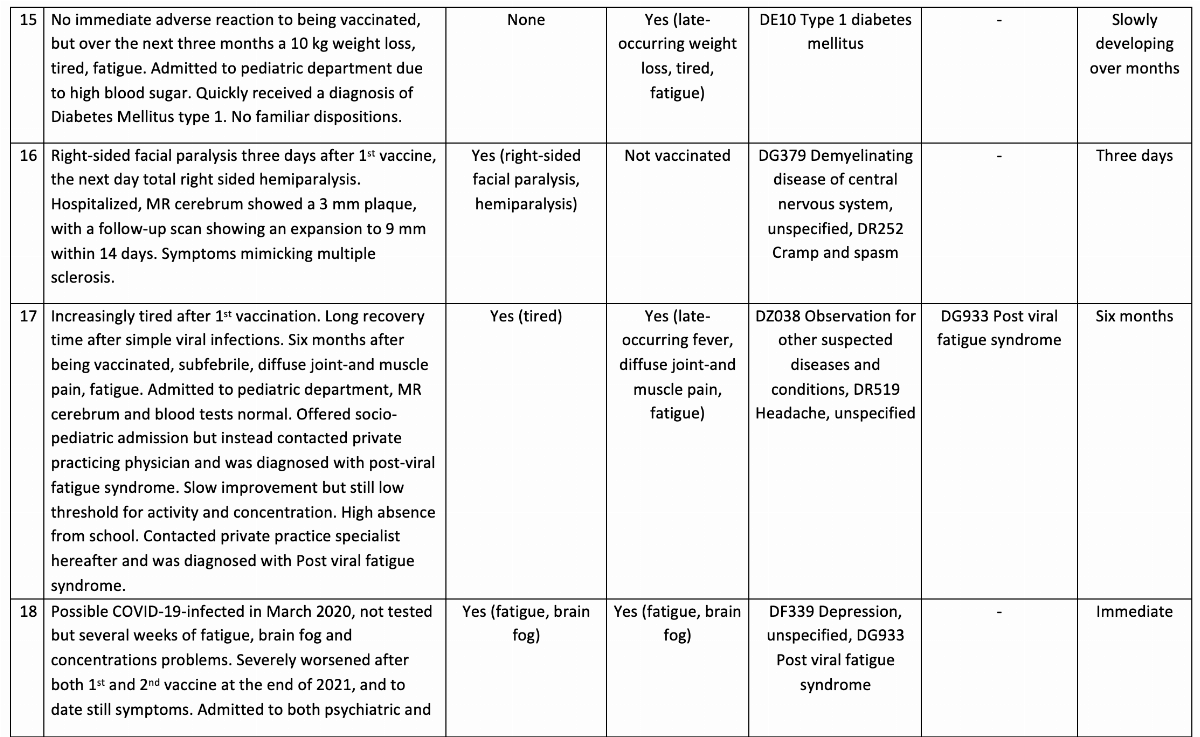
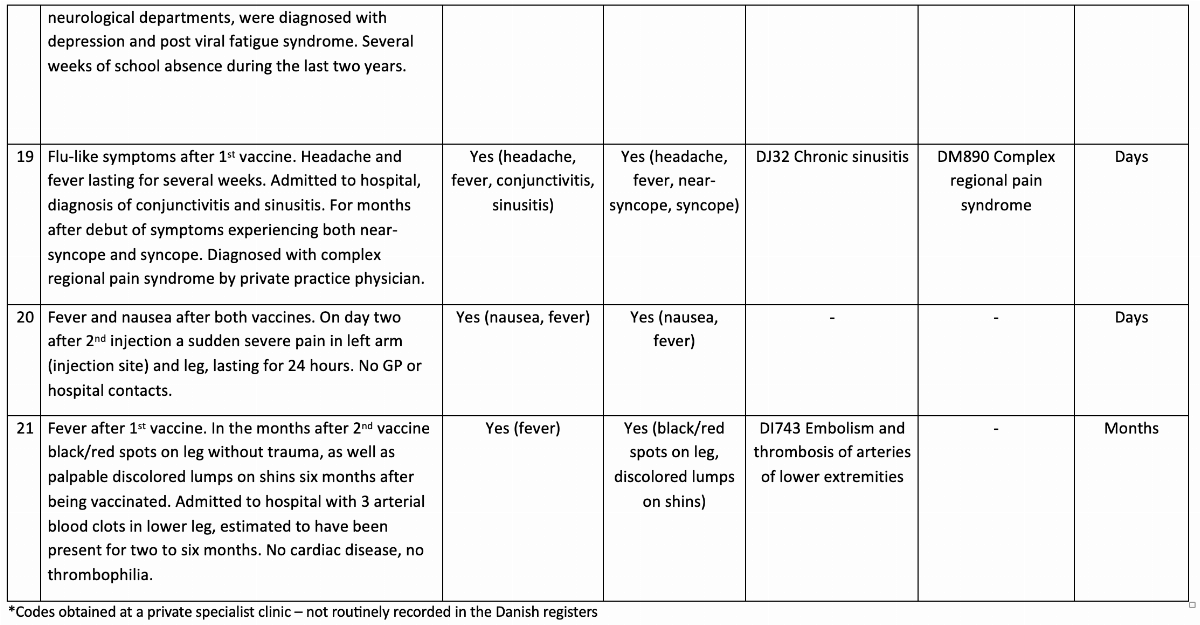
A summary of occurrence and nature of the experienced symptoms after COVID-19 vaccination, along with a presentation of the provided ICD-10 diagnoses, is presented in Table 2.
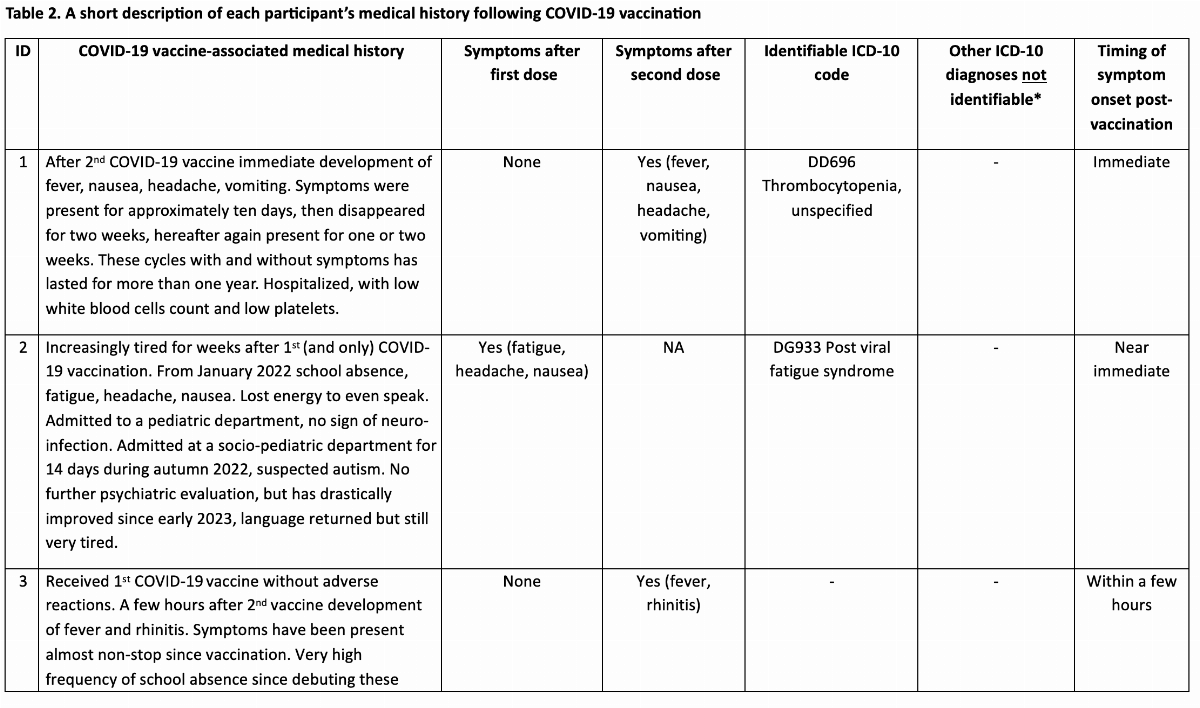
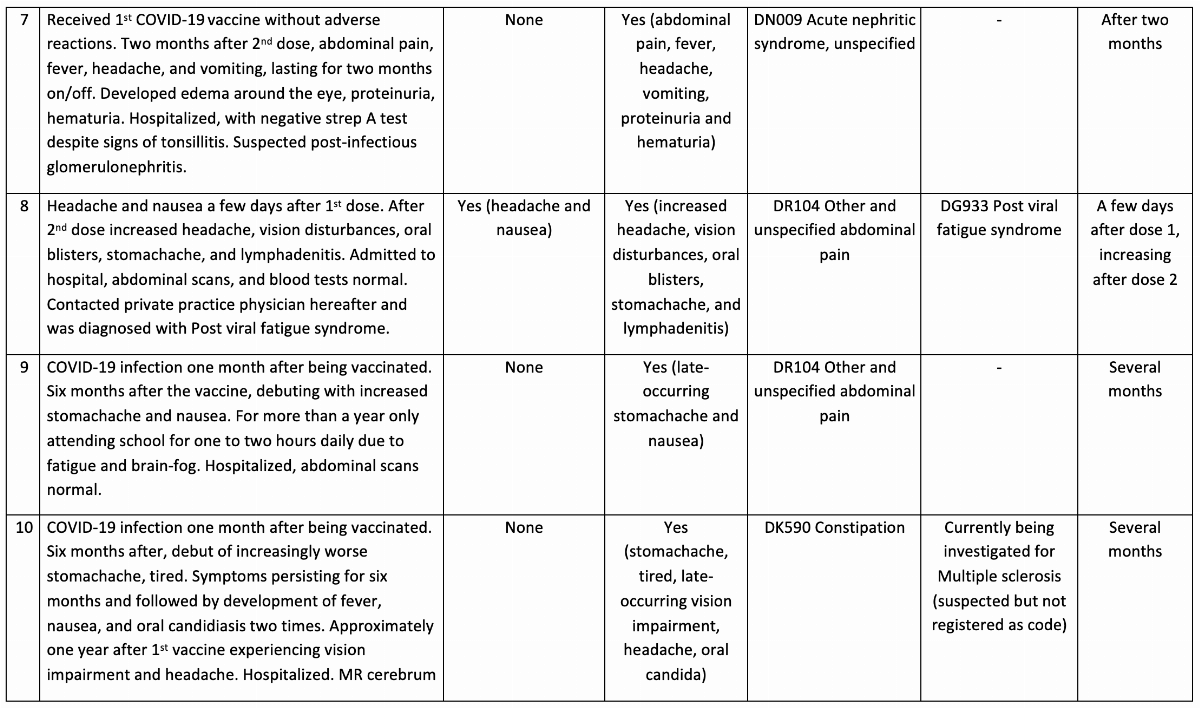
 From vaccination to debut of symptoms, the time span was broad, ranging from immediate onset of symptoms within hours or days in just over half of participants (11 children, 52%), and up to several months following immunization in the remaining ten children. Eleven children (52%) reported their adverse event following the first dose, ten following the second dose (Table 2). Eight (38%) reported worsening of a post-dose-1-event after the second dose.
From vaccination to debut of symptoms, the time span was broad, ranging from immediate onset of symptoms within hours or days in just over half of participants (11 children, 52%), and up to several months following immunization in the remaining ten children. Eleven children (52%) reported their adverse event following the first dose, ten following the second dose (Table 2). Eight (38%) reported worsening of a post-dose-1-event after the second dose.
Five children (24%, participants 1, 2, 4, 5 and 6) had a positive COVID-19 PCR test prior to vaccination. Participants 9 and 10 (10%) had a positive COVID-19 PCR test after vaccination but prior to onset of symptoms. A total of 11 children (52%) had a positive COVID-19 test months after their vaccination and first occurrence of symptoms, whereas three (14%) never tested positive for COVID-19.
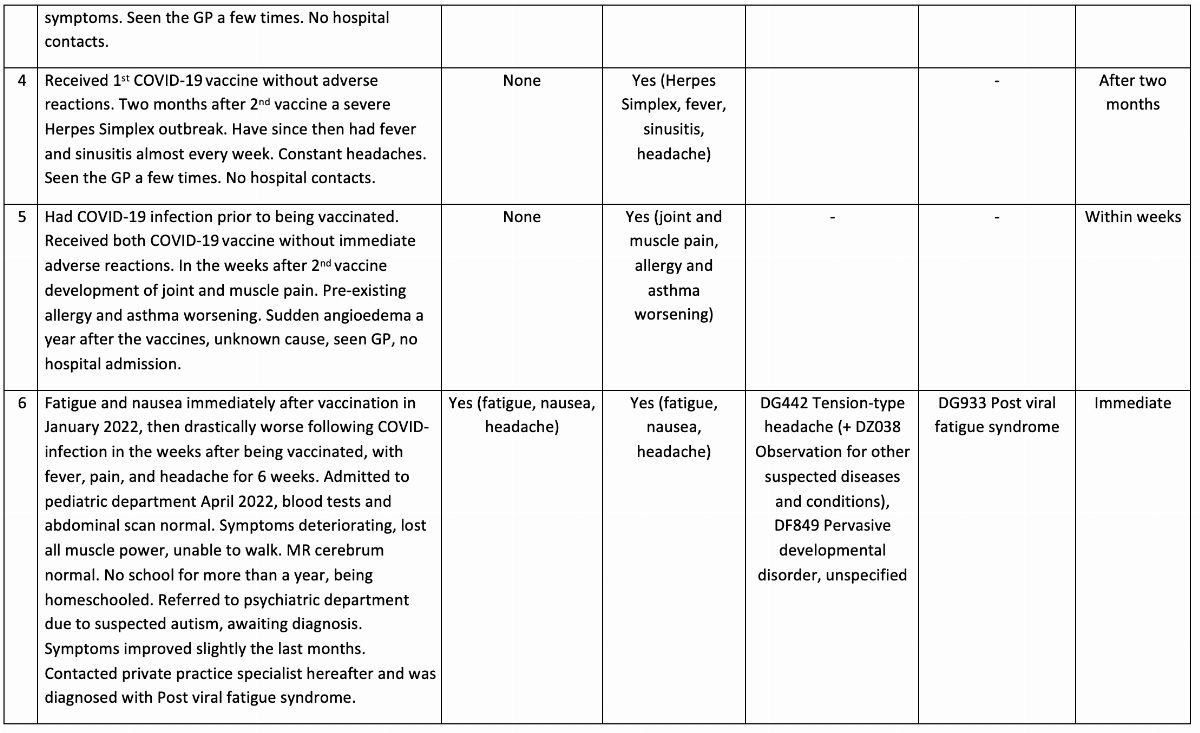
Most children (17, 81%) had at least one visit within the hospital system and thus received one or more ICD-10 diagnoses. Nine (43%) had symptoms compatible with autoimmune illnesses: demyelinating diseases (participant 10, 14 and 16), encephalitis (participant 13), endophthalmitis (participant 14), type 1 diabetes (participant 15), arterial thrombosis (participant 21), glomerulonephritis (participant 7) and idiopathic thrombocytopenia purpura (ITP) (participant 11).
The three children who at the time of the interviews were being investigated for Behçet disease (participant 14) and Multiple Sclerosis (participant 10 and 16) were not ICD-10 coded as such. Six children (29%, participants 1, 3, 4, 6, 17 and 19 ) reported symptoms of ongoing/chronic infections dominated by long-lasting fever, and a total of five children (24%, participants 2, 6, 8, 17 and 18) received a diagnosis of post-viral fatigue syndrome, a condition that may develop into myalgic encephalomyelitis/chronic fatigue syndrome (ME/CSF).18
In a post hoc supplementary analysis, we searched for published literature related to the described diseases. The results can be found in Supplementary Table 1. Seven of the diseases described by our participants and listed in Supplementary Table 1 had been registered during mRNA COVID-19 vaccine phase 3 trial in children and/or adults (demyelinating disease of CNS, type 1 diabetes, encephalitis, thrombocytopenia, chronic sinusitis, and depression).
Six conditions have been reported in post-surveillance pharmacovigilance studies (nephritic syndrome, demyelinating diseases, encephalitis, arterial embolisms, ITP, and thrombocytopenia), but without a statistically significant association. Ten conditions (including the ones described above as reported through pharmacovigilance) have been reported as single case reports or case studies. Depression has been reported in a cohort study, post-viral fatigue syndrome in an exploratory study. No published literature on pervasive development disorder was found.
Headache, fever, nausea and abdominal symptoms that were reported by seventeen participants are all common immediate adverse reactions to vaccines and were also frequently reported during the phase 3 trials.
Participants 7, 8, 13, 14, 16 and 17 all reported their newly-onset disease to the Danish Medicines Agency, and in addition, participants 13 and 16 also reported the disease to the Danish Patient Compensation. Both cases were evaluated as not being related to the vaccine.
5. Discussion
This original investigation presents a selection of potential adverse events as experienced by Danish children following COVID-19 vaccination. Most children had diseases within the autoimmune spectrum but there was no uniformity in ICD-10 diagnoses, except for the five children with a diagnosis of post-viral fatigue syndrome. Also, the time interval between vaccination and symptoms debut varied and in 24%, there was a simultaneous positive COVID-19 PCR test.
Study Limitations
This study has important limitations.
First, we used self-reported data, which can introduce information bias. This can be recall bias, where the accuracy usually deteriorates with time, and our interviews were conducted years after the time of vaccination. Selective recall is also a plausible bias, as some events are more easily remembered than others, and looking backwards might lead to the creation of causality between vaccination and the given event.19
Second, the wording of interview questions alters responses, and the answers are information that the one being interviewed perceives as sufficient but may lack information that could have been useful for the interviewer.
Third, seven children had COVID-19 vaccines and infection simultaneously, and it is important to note that many of the symptoms of both acute and long COVID-19 infection are similar to the post-vaccination symptoms,20 hence some health effects believed to be associated with vaccination may also have been associated with infection alone, both infection and vaccination, neither or both.
Vaccination and autoimmunity
While there was no clear pattern in the reported potential adverse events, a large proportion had autoimmune components. The association between vaccines and autoimmune disease is controversial.21,22 Post-vaccination autoimmune diseases have been described in the literature for vaccines against Hepatitis B, and measles, mumps and rubella (MMR), but there exist no general criteria for diagnosing vaccine-related autoimmune disease.21 A recent preprint investigated what was coined chronic post-vaccination syndrome (PVS) after COVID-19 vaccination in 241 adults. Many of the symptoms could be elicited by autoimmune diseases.23 Another recent preprint describes how 131 of 191 participants suffering from long-lasting sequelae of mRNA COVID-19 vaccination fit the ME/CSF diagnosis.24
A relationship between viral infections and autoimmunity has also been recognized, with many different trigger mechanisms, including a proinflammatory cytokine release by the innate immune system resulting in prolonged proinflammatory responses.22,25 Hence, viral infections such as Cytomegalovirus, Epstein-Barr Virus and Rubella have been associated with autoimmune diseases such as diabetes mellitus type 1 and multiple sclerosis.25 Recently it was shown that COVID-19 infection could contribute to the emergence of autoimmunity in predisposed individuals,26 and that patients with COVID-19 had increased levels of interleukin (IL) 1 and IL-6 as well as tumor necrosis factor (TNF)-α.27 These cytokines may play a role in the development of autoimmune diseases in genetically predisposed individuals.28 Proinflammatory cytokines including IL-6 were also shown to be increased following mRNA COVID-19 vaccination, indicating that an association between vaccination and autoimmune disease is plausible.29,30
Vaccination and other infections
Vaccines may have non-specific/heterologous effects, i.e. an ability to not only protect against the target disease, but also affect the risk of non-targeted infections, either beneficially or negatively, depending on vaccine type and the sex of the vaccinee.31 In the present study, six children presented with long-lasting fever, but only one had a relevant ICD-10 diagnosis (chronic sinusitis).
Consistency with phase 3 trial observations and post-marketing findings
Headache, fever, nausea and abdominal symptoms reported by 17/21 participants were already described as solicited adverse reactions during COVID-19 mRNA vaccine phase 3 trials. In the current study, these symptoms were described as long-lasting, but few participants were provided with an ICD-10 diagnosis (Table 2). A recent paper pointed out that many of the reported long-lasting adverse events after COVID-19 vaccination presented as a prolonged version of normal vaccination reactions, and this may hamper their detection, as the duration of these well-known adverse drug reactions are not easily captured in the pharmacovigilance systems and would likely be interpreted as transient adverse reactions.32
SAEs reported during the phase 3 trials in children aged 0-17 years included depression, pyelonephritis, idiopathic epilepsy (generalized), and type 1 diabetes, diseases which were also reported in this study. The descriptions of these events are not available in the clinical trials’ published main texts but can be found in either supplementary material or in the FDA/EMA reports.33,34,35
Overall, there was little evidence of association between vaccination and the symptoms described by our participants in the existing literature, as most of the published studies were case-based or showed non-significant associations (Supplementary Table 1).
Identifying rare diseases through register-based studies
The main aim of the study was to identify experienced symptoms following COVID-19 vaccination and their timing, to assess whether associations could be studied by using register data.
We found that some children were yet to receive a final or confirmed diagnosis due to the complexity of the disease pattern. Hence, only minor symptoms, such as headache or stomachache, were registered for these children although they are currently suspected of and assessed for serious diagnoses such as Behçet´s disease and Multiple Sclerosis. Thus, many register-based studies aiming to investigate associations between COVID-19 vaccines and these ICD-10 codes, often limiting themselves to diagnoses given within a certain time frame of vaccination,36 would not include these events. This highlights the importance of using different time windows in the study of potential vaccine-related adverse events.
6. Conclusion
In this original investigation, 21 cases with new-onset disease following COVID-19 vaccination were presented. A variety of diseases were described by the participants, many with an autoimmune or infectious aspect. The present study cannot establish any causal relations between COVID-19 vaccines and the observed diseases. Future register-based studies should consider combining groups of ICD-10 codes and aim to include diagnoses from specialists as well as consider different time windows following vaccination.
Funding, Disclosures & Contributions
Acknowledgements:
We are very appreciative of all parents and children who were willing to share their medical story and participate in the interviews.
A big thank you to Tracy Beth Høeg for valuable inputs to our study.
We thank Kim Lyngby Mikkelsen from the Danish Patient Compensation for providing us with information on compensation claims in Danish children following vaccination.
Ethics:
All participants provided oral and written consent to the publishing of their personal data.
Funding:
This study was funded by a grant from the Bluebell foundation. The funding agency had no role in the design of the study, data collection, analysis, interpretation or writing and publishing the results.
Data accuracy and data sharing:
All authors affirm that the manuscript is an accurate and transparent presentation of the studies being reported, and that all relevant data has been published.
Author contributions:
The study was conceptualized by CSB, SH, SMT and AP. SH conducted the interviews and wrote the first draft of the paper. SH and CBS did the literature searches. All authors approved the final version.
References
WHO. WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. 2023. Accessed July 26, 2023. https://covid19.who.int/
Our World in Data. COVID-19 vaccine doses administered by manufacturer, European Union. 2023. https://ourworldindata.org/grapher/covid-vaccine-doses-by-manufacturer
Hoffmann SS, Nielsen S, Thysen SM, Duriseti R, Benn CS. Overall Health Effects of mRNA COVID-19 Vaccines in Children and Adolescents A Systematic Review and Meta-Analysis. Published online January 18, 2024:2023.12.07.23298573. doi:10.1101/2023.12.07.23298573
Frenck RW, Klein NP, Kitchin N, et al. Safety, Immunogenicity, and Efficacy of the BNT162b2 Covid-19 Vaccine in Adolescents. N Engl J Med. 2021;385(3):239-250. doi:10.1056/nejmoa2107456
Walter EB, Talaat KR, Sabharwal C, et al. Evaluation of the BNT162b2 Covid-19 Vaccine in Children 5 to 11 Years of Age. N Engl J Med. 2022;386(1):35-46. doi:10.1056/NEJMOA2116298
Muñoz FM, Sher LD, Sabharwal C, et al. Evaluation of BNT162b2 Covid-19 Vaccine in Children Younger than 5 Years of Age. N Engl J Med. 2023;388(7):621-634. doi:10.1056/NEJMOA2211031
Ali K, Berman G, Zhou H, et al. Evaluation of mRNA-1273 SARS-CoV-2 Vaccine in Adolescents. N Engl J Med. 2021;385(24):2241-2251. doi:10.1056/nejmoa2109522
Creech CB, Anderson E, Berthaud V, et al. Evaluation of mRNA-1273 Covid-19 Vaccine in Children 6 to 11 Years of Age. N Engl J Med. 2022;386(21):2011-2023. doi:10.1056/NEJMOA2203315
Anderson EJ, Creech CB, Berthaud V, et al. Evaluation of mRNA-1273 Vaccine in Children 6 Months to 5 Years of Age. N Engl J Med. 2022;387(18):1673-1687. doi:10.1056/nejmoa2209367
Chua GT, Kwan MYW, Chui CSL, et al. Epidemiology of Acute Myocarditis/Pericarditis in Hong Kong Adolescents Following Comirnaty Vaccination. Clin Infect Dis. 2022;75(4):673-681. doi:10.1093/cid/ciab989
Sardella M, Belcher G. Pharmacovigilance of medicines for rare and ultrarare diseases. Ther Adv Drug Saf. 2018;9(11):631. doi:10.1177/2042098618792502
Onakpoya IJ. Rare adverse events in clinical trials: Understanding the rule of three. BMJ Evid-Based Med. 2018;23(1):6. doi:10.1136/EBMED-2017-110885
Thygesen LC, Daasnes C, Thaulow I, Brønnum-Hansen H. Introduction to Danish (nationwide) registers on health and social issues: structure, access, legislation, and archiving. Scand J Public Health. 2011;39(7 Suppl):12-16. doi:10.1177/1403494811399956
Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449-490. doi:10.2147/CLEP.S91125
Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 Suppl):30-33. doi:10.1177/1403494811401482
Henriksen DP, Rasmussen L, Hansen MR, Hallas J, Pottegård A. Comparison of the Five Danish Regions Regarding Demographic Characteristics, Healthcare Utilization, and Medication Use--A Descriptive Cross-Sectional Study. PloS One. 2015;10(10):e0140197. doi:10.1371/journal.pone.0140197
Statens Serum Institut. Childhood vaccination programme. Childhood vaccination programme. Accessed August 13, 2023. https://en.ssi.dk/vaccination/the-danish-childhood-vaccination-programme
O’Boyle S, Nacul L, Nacul FE, et al. A Natural History of Disease Framework for Improving the Prevention, Management, and Research on Post-viral Fatigue Syndrome and Other Forms of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front Med. 2022;8:688159. doi:10.3389/fmed.2021.688159
Althubaiti A. Information bias in health research: definition, pitfalls, and adjustment methods. J Multidiscip Healthc. 2016;9:211-217. doi:10.2147/JMDH.S104807
Scholkmann F, May CA. COVID-19, post-acute COVID-19 syndrome (PACS, “long COVID”) and post-COVID-19 vaccination syndrome (PCVS, “post-COVIDvac-syndrome”): Similarities and differences. Pathol - Res Pract. 2023;246:154497. doi:10.1016/j.prp.2023.154497
Olivieri B, Betterle C, Zanoni G. Vaccinations and Autoimmune Diseases. Vaccines 2021 Vol 9 Page 815. 2021;9(8):815. doi:10.3390/VACCINES9080815
Chatterjee S, Bhattacharya M, Saxena S, Lee SS, Chakraborty C. Autoantibodies in COVID-19 and Other Viral Diseases: Molecular, Cellular, and Clinical Perspectives. Rev Med Virol. 2024;34(5):e2583. doi:10.1002/rmv.2583
Krumholz HM, Wu Y, Sawano M, et al. Post-Vaccination Syndrome: A Descriptive Analysis of Reported Symptoms and Patient Experiences After Covid-19 Immunization. Published online November 10, 2023:2023.11.09.23298266. doi:10.1101/2023.11.09.23298266
Mundorf AK, Semmler A, Heidecke H, et al. Clinical and Diagnostic Features of Post-Acute COVID-19 Vaccination Syndrome (PACVS). Vaccines. 2024;12(7):790. doi:10.3390/vaccines12070790
Sundaresan B, Shirafkan F, Ripperger K, Rattay K. The Role of Viral Infections in the Onset of Autoimmune Diseases. Viruses. 2023;15(3):782. doi:10.3390/v15030782
Ehrenfeld M, Tincani A, Andreoli L, et al. Covid-19 and autoimmunity. Autoimmun Rev. 2020;19(8):102597. doi:10.1016/J.AUTREV.2020.102597
Qin C, Zhou L, Hu Z, et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin Infect Dis. 2020;71(15):762-768. doi:10.1093/cid/ciaa248
Masters SL, Simon A, Aksentijevich I, Kastner DL. Horror autoinflammaticus: the molecular pathophysiology of autoinflammatory disease (*). Annu Rev Immunol. 2009;27:621-668. doi:10.1146/annurev.immunol.25.022106.141627
Noé A, Dang TD, Axelrad C, et al. BNT162b2 COVID-19 vaccination in children alters cytokine responses to heterologous pathogens and Toll-like receptor agonists. Front Immunol. 2023;14:1242380. doi:10.3389/FIMMU.2023.1242380/BIBTEX
Semmler A, Mundorf AK, Kuechler AS, et al. Chronic Fatigue and Dysautonomia following COVID-19 Vaccination Is Distinguished from Normal Vaccination Response by Altered Blood Markers. Vaccines. 2023;11(11):1642. doi:10.3390/vaccines11111642
Benn CS, Fisker AB, Rieckmann A, Sørup S, Aaby P. Vaccinology: time to change the paradigm? Lancet Infect Dis. 2020;20(10):e274-e283. doi:10.1016/S1473-3099(19)30742-X
Platschek B, Boege F. The Post-Acute COVID-19-Vaccination Syndrome in the Light of Pharmacovigilance. Vaccines. 2024;12(12):1378. doi:10.3390/vaccines12121378
EMA. Assessment report Procedure No. EMEA/H/C/005735/X/0077. Published online 2021. https://www.ema.europa.eu/en/documents/variation-report/comirnaty-h-c-5735-x-0077-epar-assessment-report-extension_en.pdf
EMA. Assessment report Procedure No. EMEA/H/C/005735/X/0138. Published online 2022. Accessed August 3, 2023. https://www.ema.europa.eu/en/documents/variation-report/comirnaty-h-c-005735-x-0138-epar-assessment-report-extension_en.pdf
FDA. Vaccines and Related Biological Products Advisory Committee June 14-15, 2022 Meeting Presentation. Published online 2022. https://www.fda.gov/media/159157/download
Husby A, Hansen JV, Fosbøl E, et al. SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study. BMJ. 2021;375:e068665. doi:10.1136/bmj-2021-068665
